  先來了解正常的頭髮生長 1. 在一個時間點,大約有 90%的頭髮處於生長期,而一根頭髮的生長期大概是2-6 年。 2. 約有 10%的頭髮是處於休止期,這段休息的期間大概是 2-3 個月,休息過後頭髮即會掉落。 3. 當一根頭髮掉落時,同一毛囊會有另一根頭髮長出來取代原來的頭髮,並且開始生長期。 4. 頭髮每個月大約長 1 公分,但隨人的年齡變大,頭髮會越長越慢。 5. 大多數人掉髮是因為正常的頭髮代謝,一般每天掉 50-100 根是屬於正常現象。 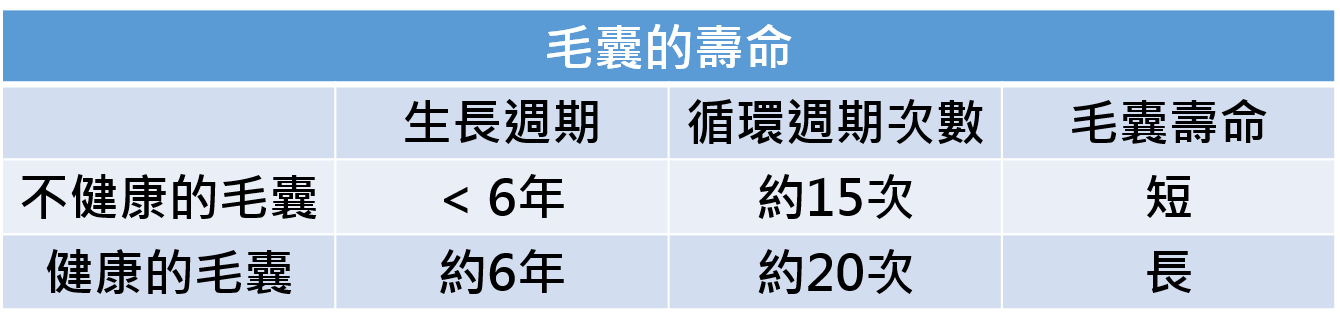 常見的掉髮迷思
1、常戴帽子或安全帽,讓頭髮不能呼吸,所以導致禿頭? A:頭髮會生長,是因為毛囊從血液中獲得氧氣與營養,所以改善頭皮的血液循環,的確可以減少掉髮的機率,但已經長出來的頭髮絕對不會「呼吸」,所以戴帽子造成的應該是悶熱導致頭皮發炎、髮質粗糙,並不是禿頭的問題。 2、每天洗頭導致掉髮? A:洗頭會掉的頭髮,是「本來就要掉的」,正常的毛髮有所謂的休止期,而洗頭時因為會清潔頭皮,容易將要掉落的頭髮順勢撥下,又能直觀看到自己頭髮在面前掉落,所以感覺好像是洗頭造成掉髮。 而有雄性禿常見的脂漏性體質,不管男女都一樣,大多是油性頭皮,髮質也多偏油性,導致他們天天洗頭、甚至一天洗好幾次,所以感覺自己是因為洗頭才掉頭髮,但其實是「倒果為因」;其實只要不是用力抓頭皮、扯頭髮,都不會影響到健康的頭髮。 3、淋一下酸雨會導致掉髮? A:一般的雨水PH值是5.6左右,酸雨定義為PH值小於5.0的雨水,也可能對皮膚、黏膜部位造成刺激跟過敏,但頭髮的毛囊是在皮膚底下,而皮膚本身就是弱酸性、也是第一層保護,這樣程度的雨水還不至於會傷害到皮膚底下的毛囊,除非跟建築物一樣24小時不停的在外面淋雨,需要長時間才有可能。 4、常梳頭會掉髮,甚至造成禿頭? A:梳頭髮會覺得容易掉髮,是因為頭髮會卡在梳子上,讓人感覺「好多」,但其實也跟洗頭一樣,只是比較容易被看到的掉髮而已,都是正常的代謝。只要不是梳子太密、或是梳頭時遇到打結的頭髮硬扯等外力影響,正常的梳頭也不會造成禿頭。 5、換坊間的生髮洗髮精,就不會再掉髮? A:洗髮精的功用是清潔頭皮與頭髮,當然有些洗髮精會添加藥性成分,能改善脂漏性皮膚炎、頭皮屑等,但對於「長頭髮」或改善「禿頭」,是沒有效的。當然治療雄性禿的時候,有人會使用生髮水 (Minoxidil,註1),雖然頭髮的數量以及重量會增加,但並無法解決雄性禿根本掉髮的問題。 目前,能從根本讓毛囊不會萎縮的藥,有兩種,分別是finasteride口服藥(例如柔沛,註2)以及 dutasteride口服藥(新髮靈,註3)。 註1:Minoxidil無法抑制雄性激素(anti-androgen)的功能,在動物體的研究中,Minoxidil並不會刺激睪固酮(testosterone)或是腎上腺雄性素(adrenal androgen)的分泌;至於在人體實驗上,血清中的睪固酮濃度也不會因為使用Minoxidil而改變。但根據臨床實驗的結果,具有雄性禿掉髮的男性和女性的頭髮,在使用Minoxidil之後,在頭髮數量及重量上,皆會明顯增加。但這種讓細小毛囊產生反轉再生的作用,尚不足以單純解釋是Minoxidil讓頭髮加快生長,似乎是Minoxidil觸發了毛囊由休止期進入生長期的關鍵所在,也因此,Minoxidil的真正作用機制,目前還是尚未釐清。 註2:finasteride口服藥是只抑制了第二型的5 α還原脢。 註3:dutasteride口服藥是同時抑制了第一型與第二型的5 α還原脢。 6、洗髮只要洗頭皮? A:頭皮一定要洗,但頭髮也不能偏廢,尤其是長髮女性,應在洗頭時好好梳理,才不會打結;如果只洗頭皮,無法達到徹底清潔的目的。 至於其他洗髮細節,不脫以下原則: 一、不一定要天天洗頭,應視個人需求及習慣,決定洗頭的頻率、次數。 二、選擇適合髮質的洗髮精。 三、用溫水沖洗乾淨,因冷水會降低洗淨力。 四、不管什麼髮質,洗頭時都要清洗乾淨,不要殘留洗髮或護髮產品在頭上。 7、洗頭時頭髮很癢,可以用指甲用力抓? A:不可用指甲,以免刮傷頭皮。洗頭時可搭配按摩3~5分鐘,可促進血液循環,此外,不管洗頭或按摩,都要使用指腹,才不會造成毛囊受傷。
0 評論
 體重超重了嗎? 可能來自身邊的人傳染給你的!!! 很多辛苦減肥的人可能根本不會想到,自己的肥胖不僅僅是因為吃得多、動得少,也很有可能是被周圍的胖親友傳染的。 2007年,耶魯大學的克里斯塔基斯教授與加州大學聖地亞哥分校醫學院醫學遺傳學教授福勒的研究團隊通過一項長時間的追蹤研究,探究了肥胖如何在人與人之間蔓延。該團隊在《NEJM 新英格蘭醫學雜誌》發表的該項研究通過對12067位有緊密社會聯繫的人進行了32年的跟蹤調查,在排除了其他可能的影響因素,如性別、隨年齡增加體重的正常增長、經濟水平的影響後發現,一個人體重的增加與否與其朋友、兄弟姐妹、配偶以及鄰居的體重增加都相關。 一個人的行為會在社交圈中產生三層影響,影響朋友,影響朋友的朋友,影響朋友的朋友的朋友。 如果你的朋友肥胖,那麼你肥胖的可能性就會高出45%; 如果你朋友的朋友肥胖,你肥胖的可能性就會高出20%; 而你朋友的朋友的朋友肥胖,則會讓你肥胖的可能性高出10%。 但你朋友的朋友的朋友的朋友肥胖,則對你影響不大了。 研究結果還發現,如果一個胖人體重增加了7.7千克,那麼他(她)朋友的體重也會相應增加2.3千克。 另外,性別也與人變胖關係密切。如果一個人的同性朋友中有一個人變胖了,他(她)體重增加的幾率也會相應提高71%。 為何胖會在社交中「傳染」? 在社交中,我們周圍的人生活飲食習慣通常會相互「傳染」。 平時我們都會有一個感覺,和要好的親戚朋友們待在一起時,很多時候會不知不覺增加飯量,要是和胖親友們在一起,可能會吃得更多。這主要是大部分肥胖人群進食速度也比一般人快,和肥胖者一起進食時,會無形中增加進食速度。而狼吞虎咽不容易產生飽腹感,這樣就會吃進更多的食物,攝入過多的熱量。 我們每個人都有從眾心理,一個人所處的圈子中一些人的群體性行為都會對自身產生影響。從心理角度來說,看到胖朋友吃得比自己還多,於是會潛意識裡認為自己稍微多吃一點也沒有什麼關係。 並且待在胖子群中,受影響的不僅僅只有吃。胖子群體一般都不愛運動,而是喜歡看電視、玩電腦、坐著聊天等一些沒有什麼運動量的活動。這樣一個人總是待在他們中間,個人活動的方式也很容易受胖友的影響而發生潛移默化的改變。比如周末喜歡宅在家裡、不愛出門活動,而這些都是導致長胖的因素。 那是不是我們就要和自己的胖朋友絕交,遠離自己的胖親屬?也沒有這麼嚴重。雖然肥胖會在胖人圈中傳染,但是並不是說和他們待在一起就一定會變胖,這主要還是取決於自己能否抵制食物的誘惑,能否堅持自己本來的生活方式。 當然,這需要較強的意志力。 如果你是一個意志堅定者,說不定還能夠帶領胖人圈中親戚朋友們一起減肥呢! 該項研究的重大價值是,讓人們認識到肥胖在社會網路中的傳播也是肥胖流行的一個重要因素。 平時積極參與健康生活方式來減緩肥胖的蔓延,因為一個人健康的改善也可能會傳播給其他人。 以下是該研究克里斯塔基斯教授再TED的演講。有興趣的朋友,可以參考看看。(有中文字幕喔!) 食品藥物管理署(以下簡稱食藥署)因應日前公費流感疫苗外觀異常事件,已依風險機制立即針對今年度後續流感疫苗檢驗封緘申請案,提高疫苗外觀檢查比例,隨即檢查到賽諾菲股份有限公司之巴斯德流感疫苗及巴斯德四價流感疫苗各一批外觀異常,判定不合格,不予封緘放行,請民眾放心。
食藥署於今年10月間分別受理賽諾菲股份有限公司1批巴斯德流感疫苗(批號R3J711V, R3J71,438,190劑,8月製造,10月上旬進口)及1批巴斯德4價流感疫苗(批號R3J721V, R3J72,80,215劑,8月製造,10月下旬進口)的檢驗封緘申請,依據中華藥典規定進行10項檢驗均合格,惟於加強外觀檢查時,發現批號R3J711V,R3J71的巴斯德流感疫苗有4支疫苗內含黑色懸浮物,批號R3J721V,R3J72的巴斯德四價流感疫苗有9支疫苗內含白色懸浮物(如附件所示),不符合中華藥典與製造廠成品檢驗規格,判定不合格,不予封緘放行,該二批疫苗依據藥事法施行細則第36條規定,須限期退運或銷毀。 所有製造或進口之流感疫苗均須依據「藥事法」法第74條及「生物藥品檢驗封緘作業辦法」規定,由食藥署派員查核貯運溫度,合格者抽取試驗或留樣所需之適量藥品,經檢驗合格者於包裝上個別加貼藥物檢查證,始得銷售。國人使用公費與自費流感疫苗皆依中華藥典規定,執行外觀、鑑別、pH值、甲醛、蛋白質含量、無菌、細菌內毒素、異常毒性、卵蛋白含量、病毒不活化及效價等共11項品質安全試驗,供國人使用之疫苗均檢驗合格,請國人安心接種疫苗。  食品藥物管理署加強管理美國及加拿大「蘿蔓生菜」輸入查驗申請
食藥署自107年11月23日至12月7日(出口日),對美國、加拿大輸入之「蘿蔓生菜」實施加強輸入管控措施,輸入必須檢附美國及加拿大食品安全主管機關證明文件,未檢附則暫停輸入查驗申請(如附件)。 食品藥物管理署(下稱食藥署)今(22)日表示, 107年11月20日美國食品藥物管理署(FDA)及疾病管制署(CDC)、加拿大公共衛生局(PHAC)發布警告指出,近期美國及加拿大發生O157:H7型大腸桿菌食物中毒病例係與食用受污染蘿蔓生菜有關,並建議美國、加拿大民眾不要食用蘿蔓生菜,且食品業者不要販賣供應蘿蔓生菜。 食藥署業已通知國內輸入、通路與餐飲業者,應落實自主管理,確認輸入、販售、供應之產品符合食品安全衛生條件,如發現有危害食品安全衛生之虞時,應依食品安全衛生管理法第7條第5項規定,主動停止製造、加工、販賣及辦理回收,並通報直轄市、縣(市)主管機關。 食藥署亦呼籲消費者家中如有已購買且尚未食用之美國、加拿大蘿蔓生菜,建議不要食用,或煮熟再食用,若有身體不適情形,應儘速就醫。 食藥署將持續觀察本事件美國、加拿大主管機關之調查情形,並請美方、加方儘速提供相關資訊且要求美方、加方應落實輸台食品源頭管理,確保產品衛生安全。 目前各大廠商處理狀況 美式賣場好市多表示,昨已收到美國公司傳來的消息,第一時間就主動將進口蘿蔓生菜預防性全面下架,另賣場內原有含蘿蔓生菜的沙拉產品,也已全數更換為美生菜,因此賣場內已未販售進口蘿蔓生菜的相關產品,目前都未接獲會員有相關不適的案例回報。 量販家樂福則表示,目前檔期販售的都是台灣蘿蔓生菜,並未有美國或加拿大進口的蘿蔓生菜,短時間內也不會進口。 愛買表示,店內目前有販售美國進口蘿蔓生菜,為讓消費者吃得安心,會進行預防性下架,改售台灣生產的蘿蔓生菜。 超市全聯指出,目前店內仍有販售美國進口的蘿蔓生菜,部分店也有沙拉產品,將全力配合政府政策,該下架就下架。 衛生福利部食品藥物管理署(以下簡稱食藥署)抽驗發現,印度Mylan Laboratories Limited所生產之valsartan原料藥,有部分批號檢出動物致癌性成分「N-亞硝基二乙胺」(NDEA),經查我國健亞生物科技股份有限公司有輸入使用,該公司並已決定自107年11月19日起,全面回收使用該原料藥來源之製劑藥品,包括「壓穩膜衣錠80毫克(衛署藥製字第056320號)」(效期111年7月30日前)及「壓穩膜衣錠160毫克(衛署藥製字第056318號)」(效期108年11月4日前)藥品。食藥署並於同日請業者即時通知醫療機構及藥局立即下架停止供應,於1個月內(107年12月19日前)完成回收,請衛生局督導下架回收事宜。另提醒正在使用該藥品的患者,該藥品主要用於高血壓等需定期服藥控制之疾病,故不建議任意停藥,應儘速回診時,與醫師討論,處方其他適當藥品。
為確保民眾用藥安全,食藥署已於107年11月12日公告NDEA及NDMA之檢驗方法,並持續主動抽驗sartan類藥品之原料藥及製劑,倘發現有異常情形,則立即採取風險管控措施。 為確保藥物安全與醫療效能,食藥署已建置藥物安全監測機制,即時監視國內、外藥物安全訊息,除設有藥物不良反應通報系統及藥物不良品通報中心之外,並對於藥物之安全性與療效亦隨時進行再評估,如醫療人員或病患疑似因使用(服用)藥品導致不良反應之發生,請立即通報衛生福利部所建置之全國藥物不良反應通報中心,藥物不良反應通報專線02-2396-0100,網站:https://adr.fda.gov.tw。如發現藥物不良品時,請立即通報衛生福利部所建置之全國藥物不良品通報中心,藥物不良品通報專線02-6625-1166分機6401,網站: https://qms.fda.gov.tw。 新聞資料詢問:陳可欣簡任技正 手機號碼:0933-927-160 辦公室電話:02-2787-7402 新聞聯絡人:洪國登科長 手機號碼:0914-091-721 辦公室電話:02-2787-7410  都免費!持健保卡「6項健檢」政府出錢 千萬別錯過
1.成人預防保健服務: 年滿40至64歲民眾,只要至健保特約醫療院所,每3年可免費健檢一次;若為35歲以上小兒麻痺患者、55歲以上原住民、或65歲以上年長者,每年皆可享有免費健檢一次的服務。 2.BC型肝炎篩檢: 凡於民國55年以後出生的民眾,於健保特約醫療院所一生可享有一次免費BC型肝炎篩檢服務。 3.口腔黏膜檢查: 年滿30歲以上有嚼檳榔(含已戒)或吸菸者,每2年可接受一次免費篩檢;若具原住民身份者,可提前至18歲開始接受每2年一次的口腔黏膜檢查。凡符合資格者, 可於健保特約具牙科、耳鼻喉科專科或其他經衛生福利部核可之醫療院所接受篩檢。 4.定量免疫法糞便潛血檢查: 年滿50至74歲民眾,可至健保特約醫療院所,每2年可接受一次免費糞便潛血檢查。 5.子宮頸抹片檢查: 年滿30歲以上女性,可至健保特約婦產科或家醫專科之醫療院所,每3年可接受免費子宮頸抹片檢查一次。 6.乳房攝影檢查: 年滿45至69歲女性,可於通過乳房X光攝影檢查認證之醫療院所檢查,每2年可免費篩檢一次;然而,若二等親內曾患乳癌之女性,則可提前自40歲開始接受免費乳房攝影檢查。 衛生福利部食品藥物管理署(以下簡稱食藥署) 於監視國際藥物安全訊息時,發現印度Aurboindo Pharma Limited公司所生產高血壓治療藥品原料藥Irbesartan含「N-亞硝基二乙胺」(NDEA)成分,該成分具動物致癌性,對人體資料尚未證實,惟為確保民眾用藥安全,食藥署立即清查所有該成分之製劑品許可證,發現健亞生物科技股份有限公司之「平壓妥膜衣錠300毫克(衛部藥製字第058235號)」使用該原料藥,該公司已於今(2)日主動啟動該藥品之回收作業(回收批號如附件)。
食藥署並於今(2)日要求業者即時通知醫療機構及藥局立即下架停止供應,並於1個月內(107年12月2日前)完成回收,請衛生局督導下架回收事宜。另提醒正在使用該藥品的患者,該藥品主要用於高血壓等需定期服藥控制之疾病,故不建議任意停藥,應儘速回診時,與醫師討論,處方其他適當藥品。 為確保藥物安全與醫療效能,食藥署已建置藥物安全監測機制,即時監視國內、外藥物安全訊息,除設有藥物不良反應通報系統及藥物不良品通報中心之外,並對於藥物之安全性與療效亦隨時進行再評估,如醫療人員或病患疑似因使用(服用)藥品導致不良反應之發生,請立即通報衛生福利部所建置之全國藥物不良反應通報中心,藥物不良反應通報專線02-2396-0100,網站:https://adr.fda.gov.tw。 如發現藥物不良品時,請立即通報衛生福利部所建置之全國藥物不良品通報中心,藥物不良品通報專線02-6625-1166分機6401,網站: https://qms.fda.gov.tw。 收錄917名雄性禿病人之跨國多中心試驗中,排除血中睪固酮濃度<250 ng/dL者,dutasteride(新髮靈)劑量為0.02、0.1或0.5mg,治療6個月後,dutasteride(新髮靈) 0.1 mg增加髮量和頭髮粗度之效果與Finasteride(柔沛) 1 mg相當,Dutasteride(新髮靈) 0.5mg增加髮量之效果較Finasteride(柔沛)高出30%。 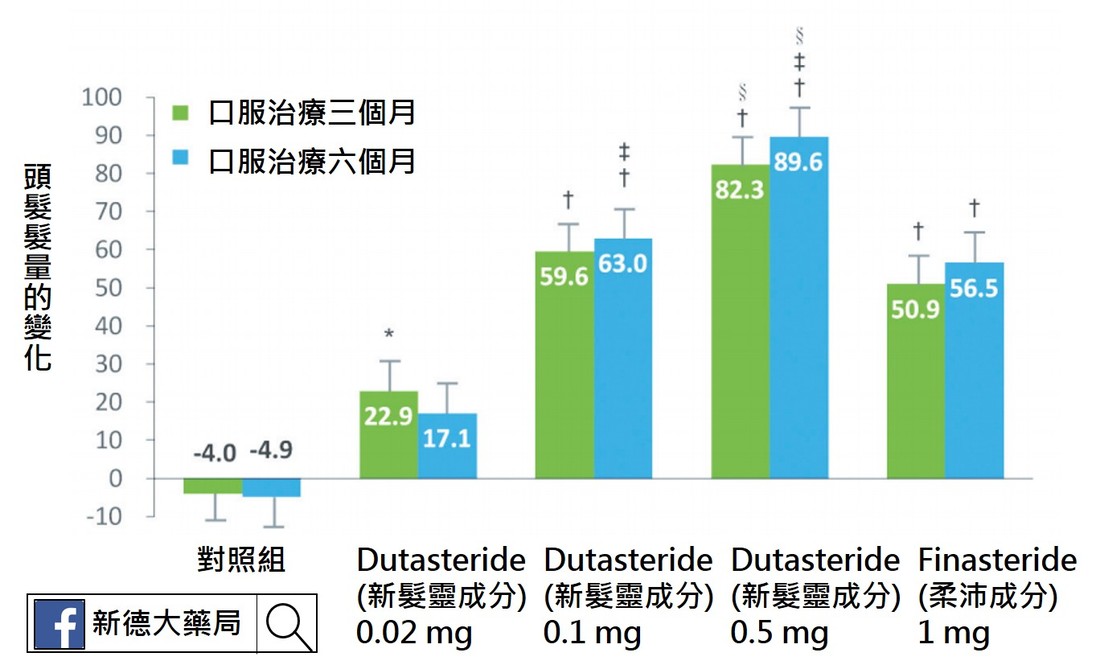 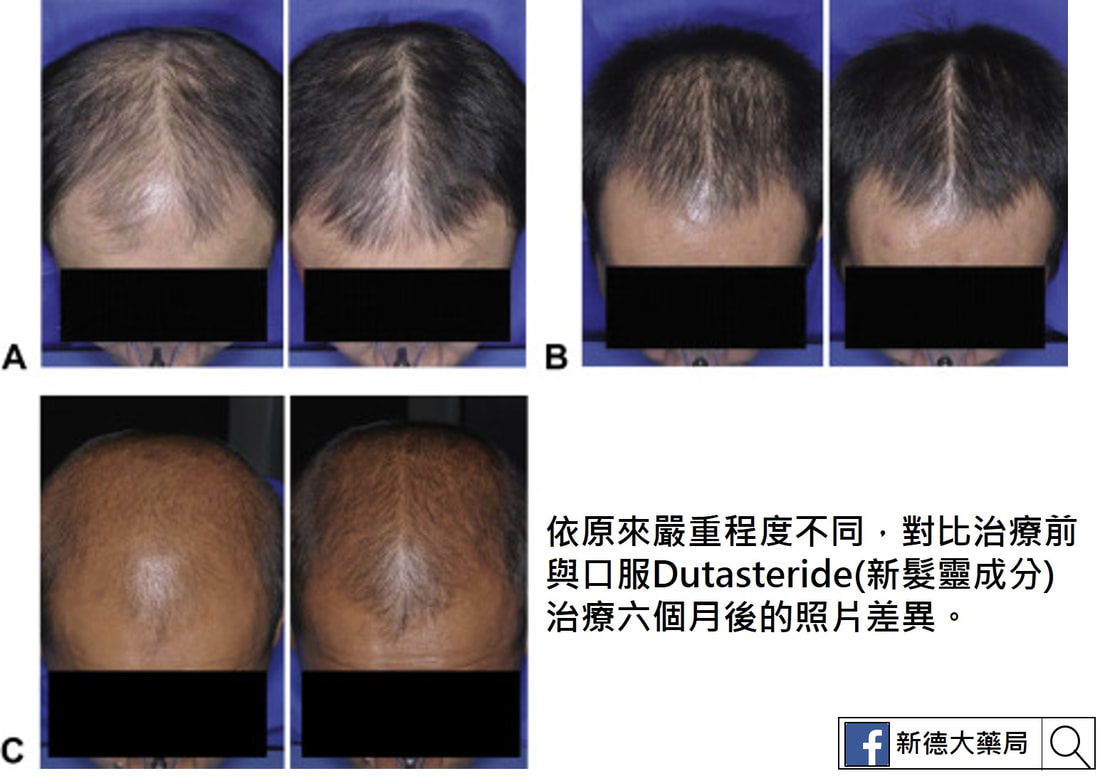 Dutasteride(新髮靈)用於不同嚴重程度的受試者,皆有一定程度之療效。
以Finasteride (柔沛)1 mg治療6個月後未達到顯著臨床效果的雄性禿病 人, 改以Dutasteride(新髮靈) 0.5 mg治療後,有77.4%達到程度不等之改善,於頭髮密度與粗度,平均改善了10.3%及19.8%。年輕的雄性禿病人經過24週治療後,使用dutasteride(新髮靈) 0.5 mg者單位面積髮量平均增加13根,使用Finasteride(柔沛) 1 mg者反而減少4根。 日本的研究以Dutasteride(新髮靈) 0.5 mg治療雄性禿病人,超過9成完成持續52週的治療,且頭頂和前額區域皆明顯改善,僅<1%受試者髮量減少。 參考文獻 1. Lee WS, Lee HJ, Choi GS, et al.: Guidel ines for management of androgenetic alopecia based on BASP classification–the Asian consensus committee guideline. JEur Acad Dermatol Venereol 2013; 27:1026-1034. 2. Eun HC, Kwon OS, Yeon JH, et al.: Efficacy, safety, and tolerability of dutasteride 0.5 mg once daily in male patients with male pattern hair loss: A randomized, double-blind, placebo-controlled, phase III study. J Am Acad Dermatol 2010; 63:252-258. 3. Tsunemi Y, Irisawa R, Yoshiie H, et al.: Long-term safety and efficacy of dutasteride in the treatment of male patients with androgenetic alopecia. J Dermatol 2016; 43:1051- 1058. 4. Marks LS: 5α-reductase: History and clinical importance. Rev Urol 2004; 6(suppl 9):S11-S21. 5. Blumeyer A, Tosti A, Messenger A, et al.: Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Dtsch Dermatol Ges 2011; Suppl 6:S1-S57. 6. Gupta M, Mysore V: Classifications of patterned hair loss: a review. J Cutan Aesthet Surg 2016; 9: 3-12. 7. Olsen EA, Dunlap FE, Funicella T, et al.: A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol 2002; 47:377-85. 8. Lucky AW, Piacquadio DJ, Ditre CM, et al.: A randomized, placebo-controlled trial of 5% and 2% topical minoxidil solutions in the treatment of female pattern hair loss. J Am Acad Dermatol 2004; 50:541-53. 9. Hillmann K, Garcia Bartels N, Kottner J, et al.: A singlecentre, randomized, double-blind, placebo-controlled clinical trial to investigate the efficacy and safety of minoxidil topical foam in frontotemporal and vertex androgenetic alopecia in men. Skin Pharmacol Physiol 2015; 28:236- 244. 10. 蔡長祐、蔡仁雨:台灣男性雄性禿之診療現況,台灣醫界,2008;51:326-330。 11. Messenger AG, Rundegren J: Minoxidil: mechanisms of action on hair growth. Br J Dermatol 2004; 150:186-194. 12. Lulic Z, Inui S, Sim WY, et al.: Understanding patient and physician perceptions of male androgenetic alopecia treatments in Asia-Pacific and Latin America. J Dermatol 2017 Mar 31. doi: 10.1111/1346-8138.13832. [Epub ahead of print] 13. Roberts JL, Fiedler V, Imperato-McGinley J, et al.: Clinical dose ranging studies with finasteride, a type 2 5alphareductase inhibitor, in men with male pattern hair loss. J Am Acad Dermatol 1999; 41:555-563. 14. Olsen EA, Whiting DA, Savin R, et al.: Global photographic assessment of men aged 18 to 60 years with male pattern hair loss receiving finasteride 1 mg or placebo. J Am Acad Dermatol 2012; 67:379-386. 15. Kaufman KD, Rotonda J, Shah AK, et al.: Long-term treatment with finasteride 1 mg decreases the likelihood of developing further visible hair loss in men with androgenetic alopecia (male pattern hair loss). Eur J Dermatol 2008; 18:400-406. 16. Rossi A, Cantisani C, Scarnò M, et al.: Finasteride, 1 mg daily administration on male androgenetic alopecia in different age groups: 10-year follow-up. Dermatol Ther 2011; 24:455-461. 17. Olsen EA, Hordinsky M, Whiting D, et al.: The importance of dual 5a-reductase inhibition in the treatment of male pattern hair loss: results of a randomized placebocontrolled study of dutasteride versus finasteride. J Am Acad Dermatol 2006; 55:1014-1023. 18. Harcha WG, Martinez JB, Tsai TF, et al.: A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia. J Am Acad Dermatol 2014; 70:489-498. 19. Jung JY, Yeon JH, Choi JW, et al.: Effect of dutasteride 0.5 mg/d in men with androgenetic alopecia recalcitrant to finasteride. Int J Dermatol 2014; 53:1351-1357. 20. Shanshanwal SJ, Dhurat RS: Superiority of dutasteride over finasteride in hair regrowth and reversal of miniaturization in men with androgenetic alopecia: a randomized controlled open-label, evaluator-blinded study. Indian J Dermatol Venereol Leprol 2017; 83:47-54. 直接看重點 近日發生之兩起流感疫苗外觀異常事件,相關批號之疫苗均已停撥停用,且截至目前未再接獲類似通報,籲請民眾勿過度恐慌。 另針對10月15日開打後至28日間曾帶幼兒至上述9個縣市合約院所接種0.25mL劑型流感疫苗的民眾,可向原接種院所確認是否接種同批疫苗, 如確認接種同批號疫苗且出現不適症狀者,可至醫療院所由醫師評估診治,如有相關疑問亦可撥打國內免付費防疫專線1922(或0800-001922)洽詢。  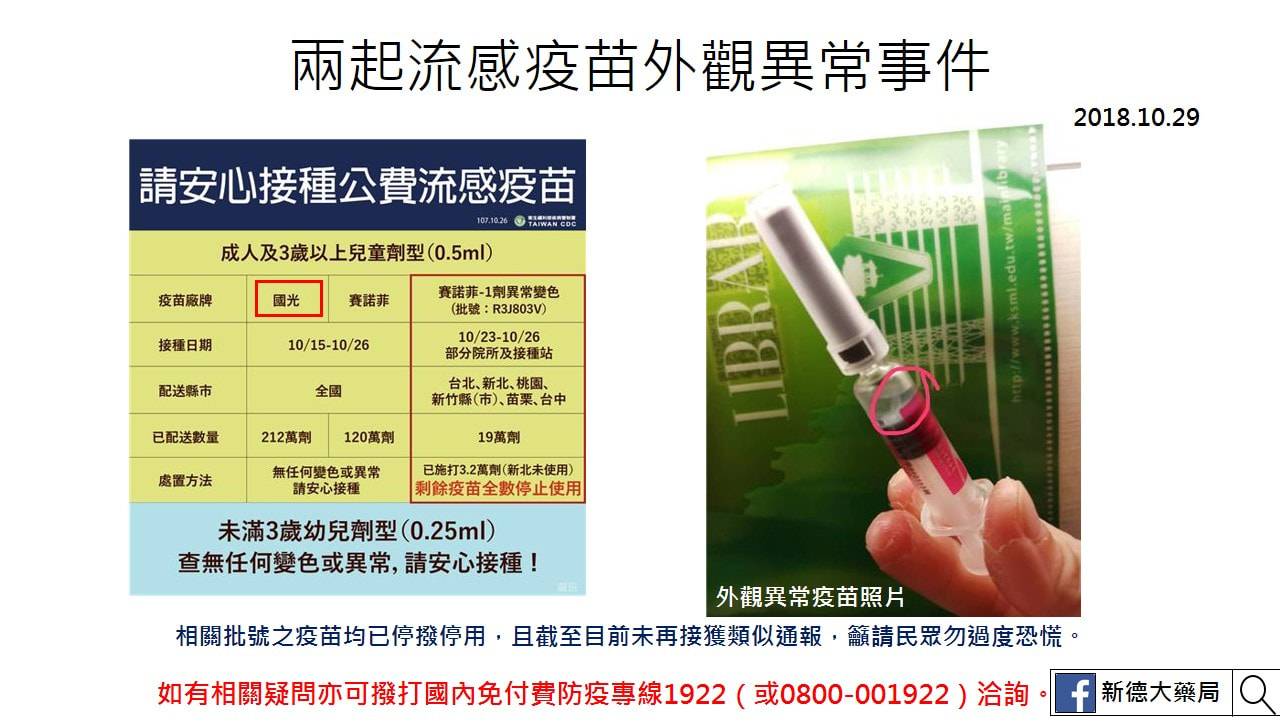 2018.10.29 疾管署接獲高雄市政府衛生局通報發現1劑有白色懸浮物之流感疫苗,同批號疫苗已暫時停撥及停用,並通報食藥署 疾病管制署今(107)年10月28日接獲高雄市政府衛生局通報該市某診所10月27日發現1劑國光公司生產之批號「FKAE1802」的流感疫苗內出現白色懸浮物。經疾管署派員檢視倉儲內未配送之同批疫苗,雖未發現其他疫苗有類似情形,為確保民眾接種安全,已通知獲配該批號疫苗之地方政府衛生局暫停撥發該批號疫苗,並轉知轄區獲配該批號疫苗之合約醫療院所,配合暫時停用該批號疫苗並檢視疫苗外觀,如有發現外觀異常等類似情形,應主動通報;截至目前並未接獲類似通報。另該批號未使用之疫苗將全數收回至衛生局所集中保管,待檢視及釐清原因後再決定是否開放該批疫苗供民眾接種。 疾管署表示,該批號流感疫苗為0.25mL劑型,共計驗收8萬2千多劑,其中已配送至9個地方政府衛生局共4萬8千餘劑,包括:臺中市、嘉義市、臺南市、高雄市、屏東縣、花蓮縣、臺東縣、澎湖縣及金門縣;另尚有約3萬4千餘劑尚未配送。因應此次通報事件,疾管署今(29)日中午12時30分邀集專家、衛生福利部食品藥物管理署、高雄市政府衛生局及疫苗廠商召開會議探討疫苗品質及接種安全;為求慎重,針對本次事件食藥署已收到廠商依藥品不良品通報機制,將儘速調查釐清。 疾管署指出,近日發生之兩起流感疫苗外觀異常事件,相關批號之疫苗均已停撥停用,且截至目前未再接獲類似通報,籲請民眾勿過度恐慌。另針對10月15日開打後至28日間曾帶幼兒至上述9個縣市合約院所接種0.25mL劑型流感疫苗的民眾,可向原接種院所確認是否接種同批疫苗,如確認接種同批號疫苗且出現不適症狀者,可至醫療院所由醫師評估診治,如有相關疑問亦可撥打國內免付費防疫專線1922(或0800-001922)洽詢。 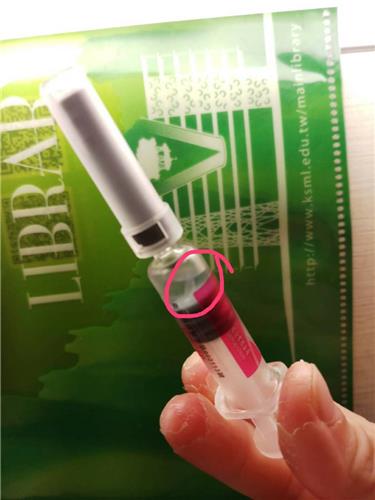 2018.10.25 疾管署針對臺北市政府衛生局通報發現1劑目測外觀明顯變色流感疫苗,已暫時停撥及停用同批號疫苗 疾病管制署今(107)年10月25日接獲臺北市政府衛生局通報該市某醫院於10月24日至社區設立流感疫苗接種站時,發現1劑目測外觀明顯變色之流感疫苗,經疾管署派員至該局及疫苗倉儲實地查看未配送之同批號疫苗,並未發現其他疫苗有類似情形。惟為確保民眾接種安全,已通知獲配該批號疫苗之7個地方政府衛生局暫停撥發該批號疫苗,並轉知轄區獲配該批號疫苗之合約醫療院所,配合暫時停用該批號疫苗並檢視疫苗外觀,如有發現變色等類似情形,請主動通報該署。目前並未再接獲類似通報。 疾管署表示,該批號疫苗共計驗收約30萬劑,已配送至地方政府衛生局共19萬餘劑,尚有10萬餘劑尚未配送。疾管署已於10月26日上午10時邀集專家、衛生福利部食品藥物管理署、臺北市政府衛生局及疫苗廠商召開會議探討疫苗品質及接種安全。另針對本次事件食藥署已要求廠商依藥品不良品通報機制,儘速調查釐清。 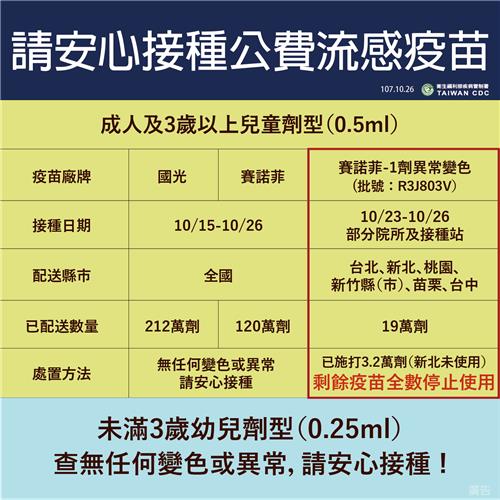  首先,來了解食物進入人體後如何運作。
食物進入身體後,經過咀嚼、胃酸的作用與小腸的消化吸收後,食物會變成食糜,食物中的營養素會在小腸吸收,進入血液循環,運送到全身;其他的食物殘渣則會繼續往下運送到大腸。水分會在大腸被回收、再利用,也就是說沒有利用價值的廢物就會在大腸脫水、並壓縮為固狀的糞便排出體外。 在正常的情況下,食物在大腸待24至36小時左右,慢慢地回收糞便中的水分與其他有用物質,所以隨著所待的時間愈來愈久,糞便會愈來愈乾,基本上,糞便會從含較多水的泥狀、半固體狀到最後變成固體狀,再排出體外。所以若很久才上一次大號,會因為食物的水分被脫乾,而使得糞便變得乾硬難排,使排便時會有痛感。此外,乾硬的糞便在推擠的過程中還可能會刮傷腸道黏膜,而使得糞便上有血絲。而糞便乾硬、排便會痛且不舒服就是所謂的便秘。 @便秘解密~認識四大項導致便秘的原因! 大體而言,之所以會出現便祕問題,有幾個原因: 一、食物體積減少導致糞便總體積不足。 在減重過程中,常因為了方便而選擇簡單、精緻的食物(例如常吃吐司、蘇打餅乾,牛奶或白水煮蛋等簡單食物);或純粹為了減重而減少食量,因而降低了食物的體積,相對的也減少了糞便的總體積,因而容易有便秘的問題。 這類便秘主要是因為糞便總體積減少的原因,所以只要增加體積量,例如:增加膳食纖維的攝取就可改善這個問題。纖維主要來自蔬菜水果,因為纖維或能吸水膨脹,或刺激腸道的蠕動,故有助排便,改善便秘、痔瘡等腸道問題,這也是為什麼一講到便秘,就會建議要多吃蔬菜水果的原因。 解決方法 多吃高纖食物:除了增加蔬菜與水果的攝取量外,五榖根莖類食物也是纖維含量很高的食物,所以可以用胚芽米或五榖米來取代白米飯,或可以煮地瓜、芋頭或紅豆湯、綠豆湯等當點心吃(使用代糖代替高熱量的砂糖)。或額外補充纖維類營養補充品。 二、腸道蠕動不佳 正常的情況下,腸道會不斷蠕動,將糞便不停的往肛門口移動。但若缺乏運動、腸道好菌太少(腸道益菌會刺激腸子蠕動)或是缺乏維生素B1等均可能降低腸道蠕動。腸道若蠕動差,會因為糞便中的水不斷被大腸脫乾,而讓糞便變得更硬,更難排,而出現便秘的情形。 解決方法 A、讓腸道益菌佔優勢:可直接補充益生菌,或攝取乳酸菌等含益菌的食物(這類食物熱量蠻高的,減肥者宜小心攝取),多吃有助好菌繁殖的食物,如寡糖類食物或纖維等。 B、多攝取能刺激腸道蠕動的食物:可多吃木瓜、香蕉、梅子、李子、蜜棗等能幫助排便的水果。或於早上起床時空腹喝梅子/李子或蜜棗汁,以刺激腸子的蠕動。 C、適度運動:運動不足會使推擠糞便所需的腹部肌肉無力,再加上腸道蠕動減弱,所以會出現即使有便意也大不出來的狀況,因此,建議增加運動量,以強化腸道的蠕動機能。 三、腸道缺乏潤滑 在減重過程中,如果水喝不夠,或因減肥而大量減少食物中油脂的攝取,都可能讓腸道因為缺乏潤滑而導致便秘。解決問題的方法就是多喝水。足量的水分可以使糞便柔軟,並可滋潤腸道,故建議每天喝2000至2500毫升的水來幫助排便,但酒精或含咖啡因的飲食會利尿,故宜少量攝取。 四、排便習慣有改進空間 很多人的便祕是因為習慣不好所致,例如:有便意時忍著不上廁所、忽略便意或飲食不均,缺乏纖維或維生素B群等營養素。基本上,排便是有一定的生理規律可循的,在某些狀況下,身體會自動產生便意,如果能利用這個生理反應,要養成規律的排便並不難。下面是兩個較容易出現便意的時候: ( 1 )當我們每天早上吃第一餐食物時,會有個所謂「胃直腸反射」,簡單地說就是只要食物進入胃,直腸(就是大腸,排便的地方)就會有反射性的蠕動反應(便意),故在早餐後,找時間去蹲廁會比較容易排便。 ( 2 )另一個產生便意的時候是在攝入一定食物的時候,只要食物堆體到一定的量,就會刺激腸道,產生便意。這也是為什麼減肥若少吃(減少食物量),很容易便秘的原因。必須注意的重點是當身體有便意時,請馬上去上廁所,不要忍著待會再說,若常常忍住或忽略便意,很容易導致便秘的產生。 解決方法 A、要吃早餐,養成規律的飲食習慣:三餐進食時間要規律,並養成吃早餐的習慣。吃早餐會有助腸道蠕動,當早餐的食物進入胃時會刺激大腸蠕動(稱胃直腸反射),而使我們產生便意。 B、不要強忍便意:因為負責讓糞便出來的肌肉群會受到大腦的控制,所以我們可以靠抑制力來強忍住便意。因此若每次有便意時,常常強忍便意的話,會使身體對腸道的刺激變得不敏感,不再將便意通知大腦,導致所謂的習慣性便秘。 如果因便祕而肚子很脹、不舒服的話,要少喝汽水、碳酸飲料、氣泡飲料等含大量氣體的飲料,或少吃容易引起腸道脹氣的食物,如花椰菜、包心菜、甘藍菜、白蘿蔔以及豆製品。  先看結論:(有興趣的朋友可以看內文更仔細一點)
目前研究指出 1、雄性禿改善程度比較:新髮靈在使用三個月或六個月後,觀察患者的頭髮密度與毛髮粗細,改善程度都比都柔沛好,甚至發現比五倍劑量的柔沛還好。(但柔沛服用超過 1mg 的正常劑量後,改善程度本來就不會隨著劑量增加而線性增加) 2、性慾減低、勃起功能降低、精子品質降低副作用比較:目前研究發現使用新法靈與柔沛皆可能會造成上述的副作用,但性功能方面的影響上,兩者並沒有顯著的差異。 3、柔沛治療效果不佳轉換到新髮靈的結果:若對於柔沛治療效果不佳,轉換使用新髮靈的話,平均髮量和厚度分別增加 10.3% 和 18.9%,皆顯著高於觀察起點。 一、Dutasteride 與 placebo 比較的臨床試驗(以最早在韓國核准用於治療雄性禿之參採臨床試驗為例)Dutasteride 於 2009 年最先在韓國核准用於治療雄性禿的適應症,其所根據的為一篇為於韓國進行為期六個月的第三期隨機雙盲安慰劑對照組臨床試驗(randomized, double-blind, placebo-controlled phase III study)。此試驗將年齡介於 18-49 歲的受試者(頭頂禿頭嚴重度介於NWH IIIv–V)分為兩組:服用 dutasteride 0.5 mg 或服用安慰劑(皆每天一次),評估其效果和安全性,主要療效指標為六個月後頭髮數量的變化。研究結果顯示,使用 dutasteride 組於六個月後平均頭髮數量於每 1 平方公分目標區域內增加 12.2 根,顯著高於使用安慰劑組的 4.7 根(p=0.0319),在次要療效指標包含專家小組及主持人對照片的評估亦達顯著差異。此外,最常見的藥物不良反應為性功能障礙(sexual dysfunction),分別在 dutasteride 組和安慰劑組佔了約 4.1% 和 2.1%,兩者並未達到顯著差異。(References 1) 二、Dutasteride, finasteride 及 placebo 比較的臨床試驗一篇第二期、隨機分配、雙盲的試驗(N=416)比較使用0.05, 0.1, 0.5 或 2.5 mg dutasteride、5mg finasteride 及安慰劑(皆每天一次)用於治療雄性禿之效益風險。受試者為 21 至 45 歲男性(頭頂禿頭嚴重度介於NWH IIIv–V),為期 24 周,主要療效指標為相較於基準值的平均頭髮增生數量(半徑 1 吋目標區域;微距攝影)。結果顯示,使用 0.05-2.5mg dutasteride 及 5mg finasteride 組,於 12 周和 24 周的平均頭髮增生數量均顯著高於安慰劑。此外,比較使用不同劑量的 dutasteride 和 5 mg finasteride,發現使用 2.5mg dutasteride 於 12 周和 24 周的平均頭髮增生數量、專家小組及主持人對照片的評估(次要療效指標),均顯著優於使用 5mg finasteride 。有關藥物引起性功能方面的不良反應大多數為輕微或中度,其中最常見的為性慾降低,在安慰劑組觀察到 2 位(3%)、0.05mg dutasteride 有 2 位(3%)、0.1mg dutasteride 有 2 位(3%)、0.5mg dutasteride 有 1 位(1%)、2.5mg dutasteride 有 9 位(13%)及 5mg finasteride有 3 位(4%)。在 2.5mg dutasteride 的 9 位,有 4 位在治療過程中恢復、2 位分別在治療結束後 3 周內及 8 周內恢復、1 位狀況並未恢復及 2 位於療程結束後失去追蹤(loss of follow-up)。 另一篇於 9 個國家(包含台灣)進行的第三期、隨機分配、雙盲的試驗(N= 917)比較使用 0.02, 0.1 或 0.5mg dutasteride、1mg finasteride 及安慰劑(皆每天一次)用於治療雄性禿之效益風險。受試者為 20 至 50 歲男性(頭頂禿頭嚴重度介於NWH III–V;排除前額禿), 觀察期間為 24 周,主要療效指標為於 24 周時,相較於基準值的平均頭髮增生數量(半徑 2.54 公分於頭頂之目標區域;微距攝影)。結果顯示,於 24 周時,相較於基準值之平均頭髮增生數量,使用 0.1、0.5mg dutasteride 及 1mg finasteride 組,皆顯著高於於安慰劑組(all p<.001);而 0.02mg dutasteride 僅在 12 周時顯著優於安慰劑,24 周時則無顯著差異。 另比較不同劑量 dutasteride 和 1mg finasteride,只有使用 0.5mg dutasteride 於 12 周和 24 周時顯著優於 1mg finasteride。另在次要療效指標方面,0.5mg dutasteride 在相較於基準值的平均頭髮增生數量(半徑 2.54 公分)、頭髮寬度 (hair width) 變化量、專家小組及主持人對照片的評估,於 24 周時均顯著優於 1mg finasteride。 此外,與性功能相關的不良反應,最常見的為亦為性慾改變/降低,在安慰劑組觀察到 3 位(1.7%)、0.02mg dutasteride 有 15 位(8.1%)、0.1mg dutasteride 有 13 位(6.9%)、0.5mg dutasteride 有 9 位(4.9%)、及 1mg finasteride 有 12 位(6.7%)。此研究並無觀察到 dutasteride 劑量和發生性功能方面不良反應之關係,整體亦無發現有關攝護腺癌、男性乳癌及心血管的不良反應。Amory 等人進行隨機分配、雙盲試驗研究 5mg finasteride(n=34)、0.5mg dutasteride(n=33) 及安慰劑(n=32)每天一次,使用 1 年,對二氫睪酮(dihydrotestersterone)的濃度及精子生成(spermatogenesis)的影響。受試者為健康男性,研究結果顯示,finasteride 組和 dutasteride 組,相較於安慰劑組,於第 26 周及第 52 周時與基準值比較,皆顯著降低二氫睪酮(dihydrotestersterone)的濃度(finasteride:-70.3 及 -72.7%; dutasteride:-93.8 及 -93.3%),而在停藥之後,finasteride 組和 dutasteride 組中的二氫睪酮濃度皆回到觀察起點,然 finasteride 組恢復速度較 dutasteride 組快(停藥後 8 周 vs. 12 周)。在療程 24-28 周時,finasteride 和 dutasteride 組的精蟲數(sperm count),與基準值比較皆顯著低於安慰劑組(finasteride:-34.3%; dutasteride:-28.6%),但於 52 周(finasteride:-16.2%; dutasteride:-24.9%)及停藥後 24 周時(finasteride:-6.2%; dutasteride:-23.3%)並無顯著差異。此研究可以看出使用 0.5 mg dutasteride 或 5mg finasteride 會影響血清二氫睪酮的濃度及精子生成,但影響非不可逆,又以 5mg finasteride 恢復速度較 0.5mg dutasteide 更快,原因可能為 finasteride 半衰期為 6-8 小時,而dutasteride 的半衰期則為 4 周。(References 2,3,4) 三、Finasteride switch to dutasterideJung 等人5收納輕度至中度雄性禿使用 finasteride 1 mg/d 至少 6 個月但療效不佳者當受試者(N=35),給予 0.5mg/d dutasteride 24 周,觀察其療效和風險。療效指標為專家對照片整體評估結果及利用自動數位影像計數評估的髮量和厚度(hair density and thickness)。結果顯示,在所有 31 位受試者完成試驗中,有 24 位(77.4%)髮禿狀況優於觀察起點,7 位(22.6%)則無顯著差別;平均髮量和厚度分別增加 10.3% 和 18.9%,皆顯著高於觀察起點。此研究觀察到 6 位受試者(17.1%)有性功能方面(性慾降低、勃起障礙和射精障礙)的不良反應。此篇研究結論使用 finasteride 治療雄性禿 6 個月但無療效的患者可換成使用 dutasteride,然而因為觀察到 dutasteride 發生性功能不良反應比率高於 finasteride,建議 dutasteride 為治療雄性禿為第一線療法,於目前恐還言之過早。另外,此研究的限制(limitation)之一為無繼續使用 finasteride 的對照組,觀察到療效可能部分為 finasteride 的效果,因此仍需要研究去探討當使用 finasteride 多久沒有觀察到療效時適合換成 dutasteride。(References 5) 四、系統性文獻回顧及統合分析(systematic review and meta-analysis)一篇統合分析收集了 16 篇有關 0.5 mg dutasteride、1mg finasteride 或 5mg finasteride 用於治療雄性禿的臨床試驗,進行效益風險評估。其結論為 0.5 mg dutasteride、1mg finasteride 和 5mg finasteride 組別之間療效和發生性功能障礙之副作用並無差異, 與安慰劑相比,產生性功能障礙之副作用亦無差異。 Liu 等人收集了 17 篇 5α-reductase inhibitors 用於治療雄性禿(AGA)及攝護腺肥大(BPH)的臨床試驗,進行有關性功能不良反應之統合分析。其研究結果顯示,相較於安慰劑,5α-reductase inhibitors 用於治療 BPH 時發生性功能障礙、勃起障礙或性慾降低的風險(pooled RR)分別顯著高於安慰劑;然而用於治療 AGA 時則皆無顯著差異。此外,次群組分析中(subgroup analysis)發現,治療 BPH 時,相較於安慰劑,dutasteride 發生性功能不良反應的風險高於使用 finasteride (RR=4.09, 95%CI=1.03-16.31 vs. RR=1.54, 95%CI=1.02-2.32);而治療 AGA 時,相較於安慰劑,使用 finasteride 或 dutasteride 皆無顯著差異,且不同劑量的 finasteridec 或 dutasteride、療程長短發生相關風險亦無顯著差異。 (References 6,7) References 1.Eun, H. C. et al. Efficacy, safety, and tolerability of dutasteride 0.5 mg once daily in male patients with male pattern hair loss: A randomized, double-blind, placebo-controlled, phase III study. J. Am. Acad. Dermatol. 63, 252–258 (2010). 2.Olsen, E. A. et al. The importance of dual 5α-reductase inhibition in the treatment of male pattern hair loss: Results of a randomized placebo-controlled study of dutasteride versus finasteride. J. Am. Acad. Dermatol. 55, 1014–1023 (2006). 3.Gubelin Harcha, W. et al. A randomized, active- and placebo-controlled study of the efficacy and safety of different doses of dutasteride versus placebo and finasteride in the treatment of male subjects with androgenetic alopecia. J. Am. Acad. Dermatol. 70, 489–498 (2014). 4.Amory, J. K. et al. The effect of 5α-reductase inhibition with dutasteride and finasteride on semen parameters and serum hormones in healthy men. J. Clin. Endocrinol. Metab. 92, 1659–1665 (2007). 5.Jung, J. Y. et al. Effect of dutasteride 0.5 mg/d in men with androgenetic alopecia recalcitrant to finasteride. Int. J. Dermatol. 53, 1351–1357 (2014). 6.Gupta, A. K. & Charrette, A. The efficacy and safety of 5α-reductase inhibitors in androgenetic alopecia: a network meta-analysis and benefit-risk assessment of finasteride and dutasteride. J. Dermatolog. Treat. 25, 156–61 (2014). 7.Liu, L. et al. Effect of 5α-Reductase Inhibitors on Sexual Function: A Meta-Analysis and Systematic Review of Randomized Controlled Trials. J. Sex. Med. 13, 1297–1310 (2016). 三十五歲的王姓粉領族,從小視力好、沒戴過近視眼鏡,今年九月時,除了上班要盯電腦螢幕,下班後還瘋狂追劇,一口氣熬夜三天看完七十集的宮鬥劇《延禧攻略》,突然發現眼睛看近物時模糊、吃力,趕緊到眼科檢查,才發現調節水晶體的「睫狀肌」收縮出現遲滯,年紀輕輕就確診罹患老花眼。 控制看遠近「睫狀肌」 收縮遲滯 王小姐從小視力一直維持在一.二,上班後因常看電腦,有時眼睛痠痛會自行點眼藥水,但上月追完劇之後,發現看近物很模糊,到眼科檢查,醫師發現她控制看遠近的「睫狀肌」收縮已出現遲滯。 老花眼成因是眼睛內的水晶體,隨年紀增長變得渾濁僵硬,負責調節水晶體的「睫狀肌」無力,造成眼睛肌肉要花更大力氣調節對焦,容易出現眼部疲勞、失焦或眼窩脹痛、頭部疼痛等症狀。 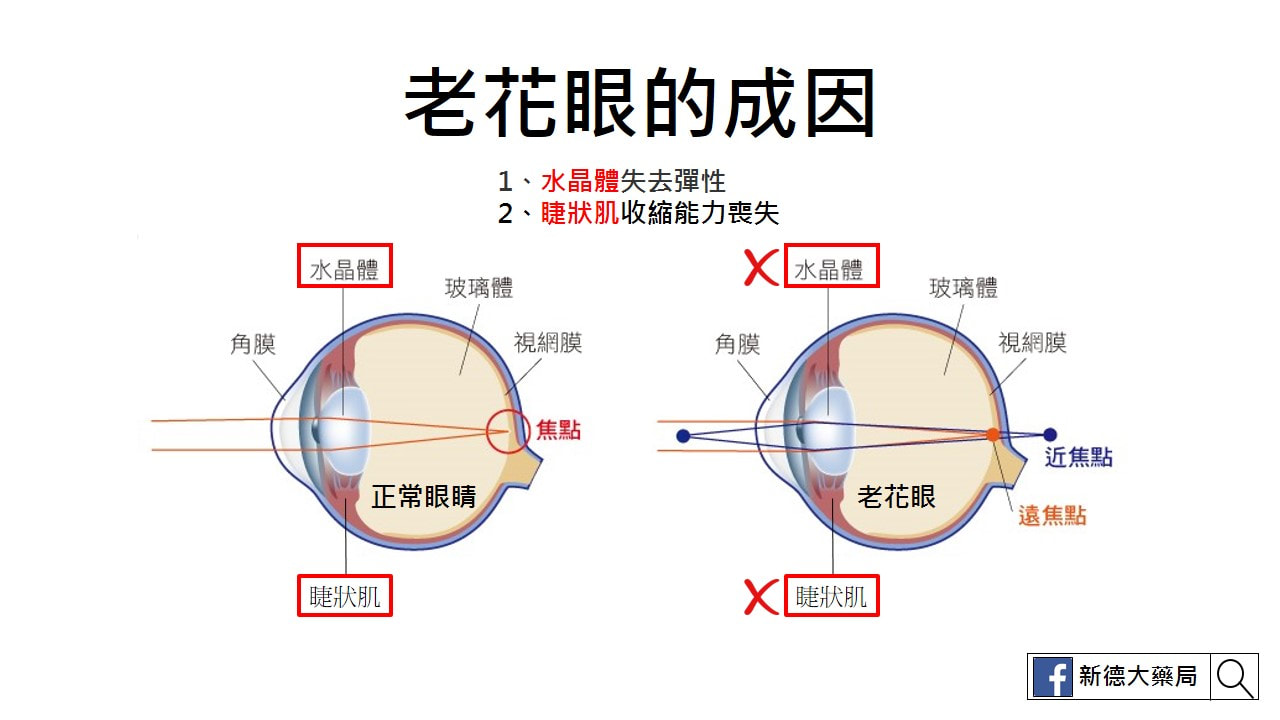 短期眼睛過度疲勞 提前出現老花 一般民眾約在四十歲會出現一百度的老花,隨著3C產品盛行,不少四十歲以下的民眾,因用眼過度提前出現老花,這名患者就是因短期內眼睛過度疲勞,出現老花眼。 用眼過度出現短暫視力模糊的患者,通常只要恢復正確用眼習慣,讓眼睛充分休息,就會慢慢恢復正常,但若是因年紀大、「睫狀肌」失去彈性,即使休息也無法恢復。薛維禎提醒民眾,應避免近距離、長時間看電腦、電視、手機,最好每看三十分鐘就休息十分鐘,並看看五、六公尺遠以外的東西,讓眼睛充分休息。 那很多人會問,補充什麼保健食品有幫助呢? 老花眼是因為 1、水晶體失去彈性 2、睫狀肌收縮能力減退 因此,主要還是要多讓眼睛時常看近看遠的訓練睫狀肌,就像練肌肉一樣,光只吃保健食品,就可以強壯肌肉嗎?答案當然是不行。 記得每看三十分鐘近物(手機、平板或電腦),就休息十分鐘,看看武、六公尺以外的東西,才能讓眼睛的睫狀肌休息。 至於補充眼睛保健食品,我們可以參考針對眼睛疲勞的保健食品, 葉黃素、蝦紅素、魚油及花青素都能有助於改善眼睛疲勞的狀況,也就是說能抑制水晶體曲折度的退化,舒緩睫狀肌的緊張。 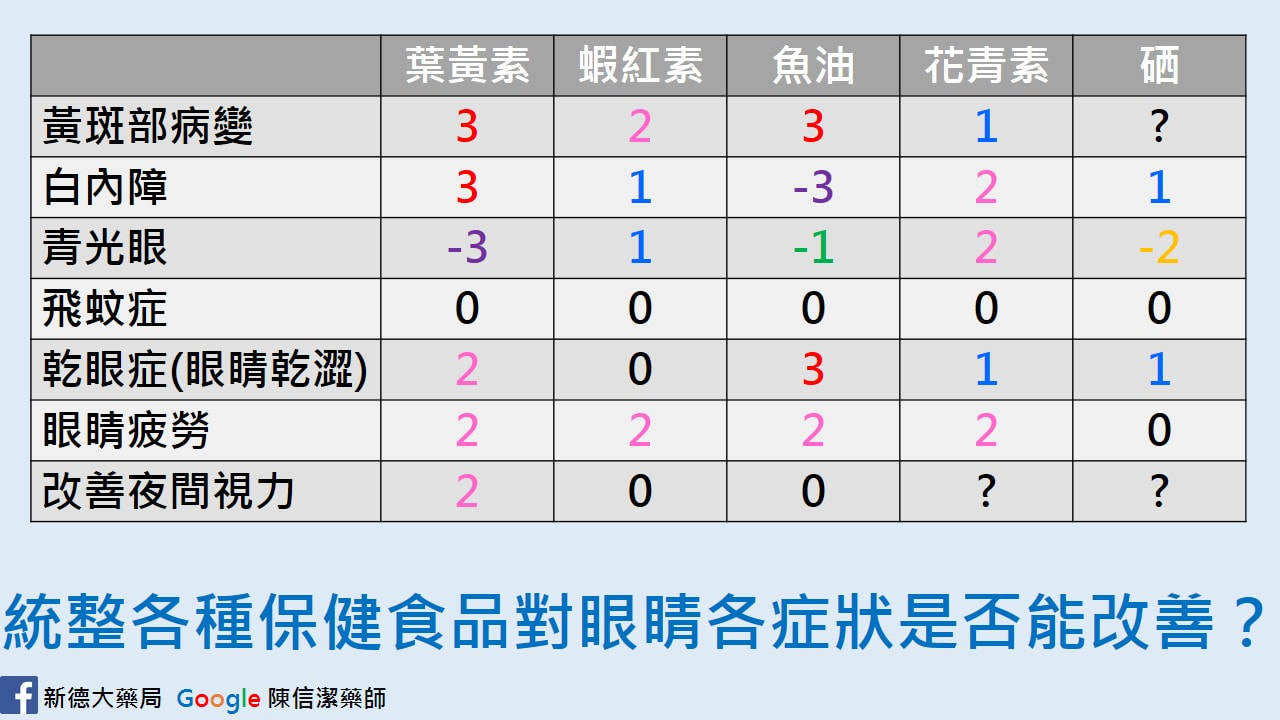 「世界關節炎日(World Arthritis Day)」,是在1996年,由歐洲的國際風濕及關節炎協會(Arthritis and Rheumatism International,ARI)所創立,在這類疾病中,以類風濕性關節炎最為嚴重,被稱為不死癌症,以下就介紹類風濕性關節炎和風濕性關節炎的不同之處,以及治療發展。  先來看看類風濕診斷的標準。 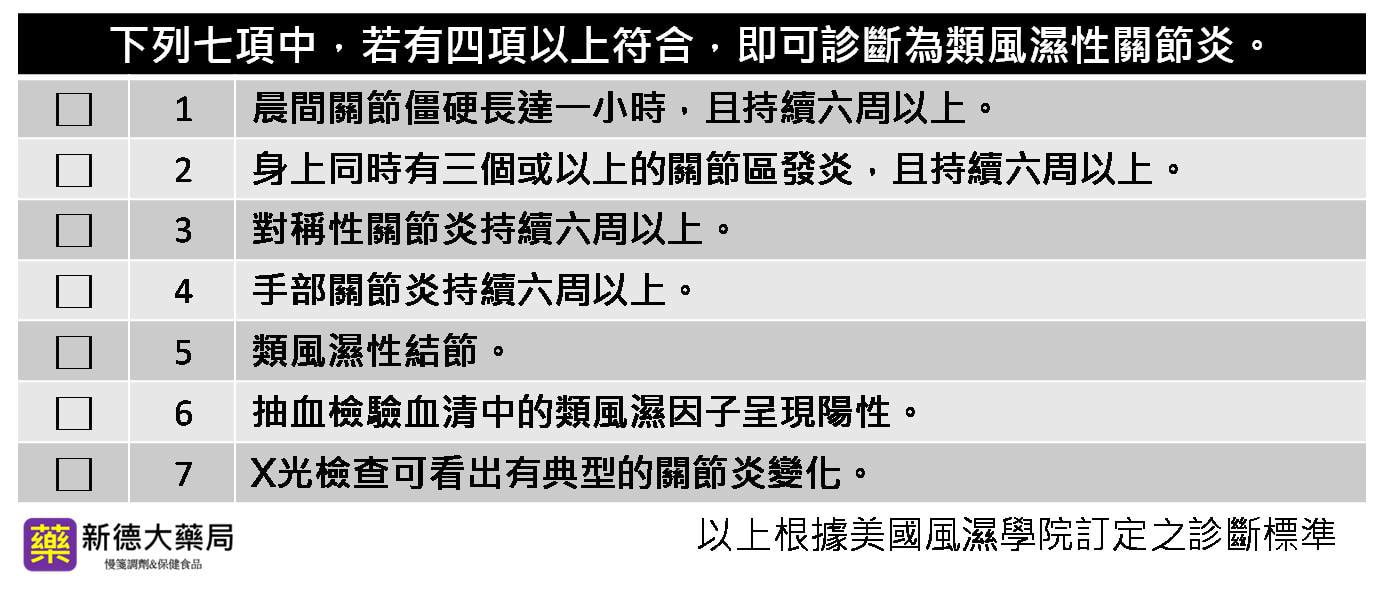 風濕性關節炎和類風濕性關節炎有什麼不同?
風濕性關節炎是一種引起骨關節疼痛的輕微炎症,也稱為骨關節炎或關節變性病,主要發作於膝關節、腰椎等大關節的部位;而類風濕性關節炎的成因不明,是一種自體免疫攻擊造成全身發炎的病症,除了大關節外,也容易侵襲手腳的小關節,導致關節變形,並有對稱性的特點,而且罹患此病,將終生為之所苦,無法痊癒只能緩解症狀,嚴重者可能殘廢。 類風溼性關節炎的藥物治療 目前類風溼性關節炎的治療選擇有一線的止痛藥、非類固醇抗發炎藥(NSAID)、疾病修飾抗風濕藥物(DMARDs)和二線的生物製劑(Biologics)及小分子口服藥物等。 一線藥物: 非類固醇抗發炎藥(NSAID)具有具有解熱鎮痛的效果,可緩解患者不適,但通常會有胃潰瘍和胃病變的副作用;而疾病修飾抗風濕藥物(DMARDs),有許多不同的藥物機轉,提供醫師依照患者病情選擇,阻止器官受到自體免疫系統的進一步破壞。 二線藥物: 生物製劑 (Biological Agents),是由生物科技所研發出來的蛋白質製劑,以注射的方式抑制體內發炎反應物質,其功能和DMARDs一樣可以調節免疫,但部會影響正常細胞的運作,屬於選擇性的免疫抑制劑。 但臨床上發現有少數患者,使用這類生物製劑後有B型、C型肝炎病毒再活化或出現結核病感染的風險問題。 而小分子口服藥物,是阻斷體內發炎激素生成的訊息傳導路徑(JAK路徑),可以直接抑制體內發炎激素的生成,降低發炎反應,是一種新的治療選擇。 目前類風濕性治療的方式很多,經衛福部規定,患者需要先使用一線藥物3~6個月以後,才能申請選擇注射大分子的生物製劑或口服小分子藥物治療。 小分子口服藥物從2014通過健保給付,今年的劑型也從一天服用2顆,變成一天服用1顆,使患者更便利控制類風溼性關節炎病情,在提升日常生活的品質,有很大的幫助。 不管增肌還是減脂,吃在這個過程中非常重要。 尤其是早餐,不但要吃,還要吃好。 國外健身較為普遍,他們的減脂餐有許多我們可以藉鑑的地方,下面是一位健身達人的減脂餐,正在減重的可以參考一下喔! 三分練、七分吃。吃錯再怎麼運動都很難瘦,很難減脂!
 維他命D能提高人體腸道吸收鈣質的能力, 而維他命K則能活化骨細胞的羧化作用,增加骨質與鈣的結合,增加骨質密度,進而幫助鈣質留在體內。 簡單來說就是,維他命D是幫助把鈣拉進體內,維他命K則是把鈣拉進骨頭內。 因此,預防骨折的關鍵是在骨頭,也就是骨頭內的鈣質不夠就容易造成骨折, 所以,重點在於如何把鈣拉進骨頭,也就是要靠維他命K把鈣拉進去骨頭,才能增加骨頭的鈣質。   先說結論,不是吃地瓜就能瘦啊!! 先來看看地瓜的營養成分(每一百公克) 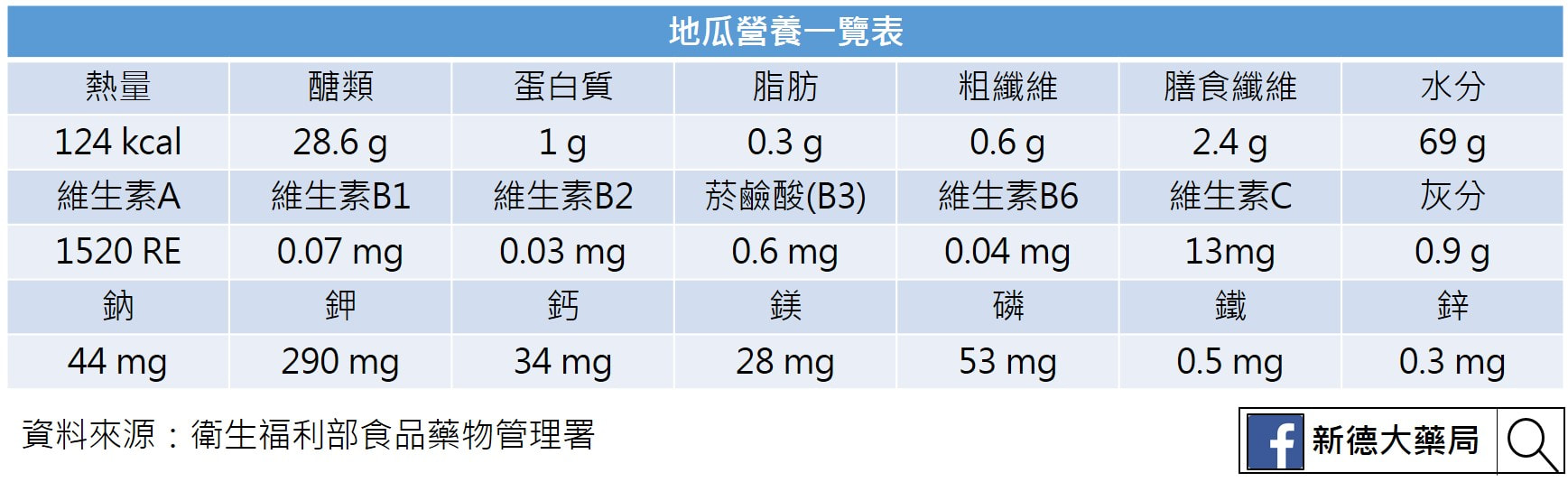 從基本營養素的角度來看,地瓜的最大亮點就是纖維!每100公克有2.4公克。
纖維,在澱粉類食物中算是很很好的,吃一條200公克的地瓜就可吃到4.8公克纖維,達到每日建議纖維攝取量的1/6左右。 從維生素的角度來看,地瓜有非常好的維生素A來源! 每100公克含1520RE的維生素A,是同量番茄的18倍,想要補充維生素A者很好的食物選擇。雖然每100公克也含13毫克維生素C,但因維生素C會溶於水,對光熱(溫度)很不穩定,而地瓜一定要經過烹調才能食用,所以,地瓜不是好的維生素C食物選擇。 從礦物質的角度來看,地瓜是鉀的良好來源!每100公克含290毫克鉀,而一般地瓜一條約200~300重,吃一條就可吃鄏600~700公克鉀,故可說是很好的鉀來源食物,想要補充鉀的人固然可多吃地瓜,但需要限制鉀的人也要留意它的攝取。 總結上述,從營養的角度來看,地瓜為屬於非精緻澱粉食物、富含纖維、維生素A及鉀的食物,相較於一般我們日常所吃的澱粉類食物(飯、麵、麵包吐司等)來說,地瓜可說是相當好的一個營養又健康的澱粉類食物! 到底吃地瓜不是就能減重呢? 首先,來看看地瓜的熱量到底高不高。 每100公克124大卡,這是什麼意思呢?如果讓我們換成用食用量來看的話,以現在最夯的烤地瓜來看,小一點,約半個手掌大小的,大概就有超過300大卡的熱量,比一碗飯熱量還高。重點是,吃這樣一條地瓜並不會飽,吃個兩條熱量則可媲美一個便當或一餐,所以從熱量的角度來看吃地瓜是無法減肥的,你只會覺得吃得很委屈(這是烤的,又只吃這麼一小條,為什麼吃這麼少還是不會瘦?!),甚至還會因此而吃胖!以一般1200大卡控制熱量的減肥飲食來看,一天只能吃四條地瓜而已! 可是很多人說地瓜是低GI的食物,不是吃低GI的食物比較不會胖嗎? 錯。低食物GI值低≠吃不胖。 地瓜的升醣指數(GI)值約55。 所謂GI值是用來檢測食物吃到體內對血糖的波動大不大,若吃一個食物會讓血糖快速上升,就會促使身體分泌較多的胰島素出來將這些多餘的糖帶到細胞儲存,故會有所謂食物的GI值越高,越容易刺激胰島素,使熱量轉變為脂肪而變胖;GI值低則較不易變胖的說法。 實際上,會不會胖與熱量多不多有關,和GI值沒有絕對關係,舉例來說油脂和肉類食物GI值很低(因為這類食物含醣份低,故吃了後血糖不會快速上升,故GI值很低)。 但吃多了還是會胖;而低GI值的澱粉類食物你若吃太多也會胖。 要說低GI食物對減肥的幫助,頂多是說它必較不會引起血糖波動,故較不會刺激食慾而已。 那減重到底可不可以吃地瓜? 可以。 基本上,地瓜是一個營養價值蠻高的澱粉類食物,GI值不高,且富含纖維,很適合規劃到減肥飲食中,取代原本所吃、營養價值較低的米飯、麵包、吐司之類的主食。 但不要為了減肥而以地瓜為正餐(因為吃一條不會飽,吃兩條熱量太高),或聽說吃地瓜可以減肥而拿地瓜當點心吃;或為了減肥而只吃地瓜。 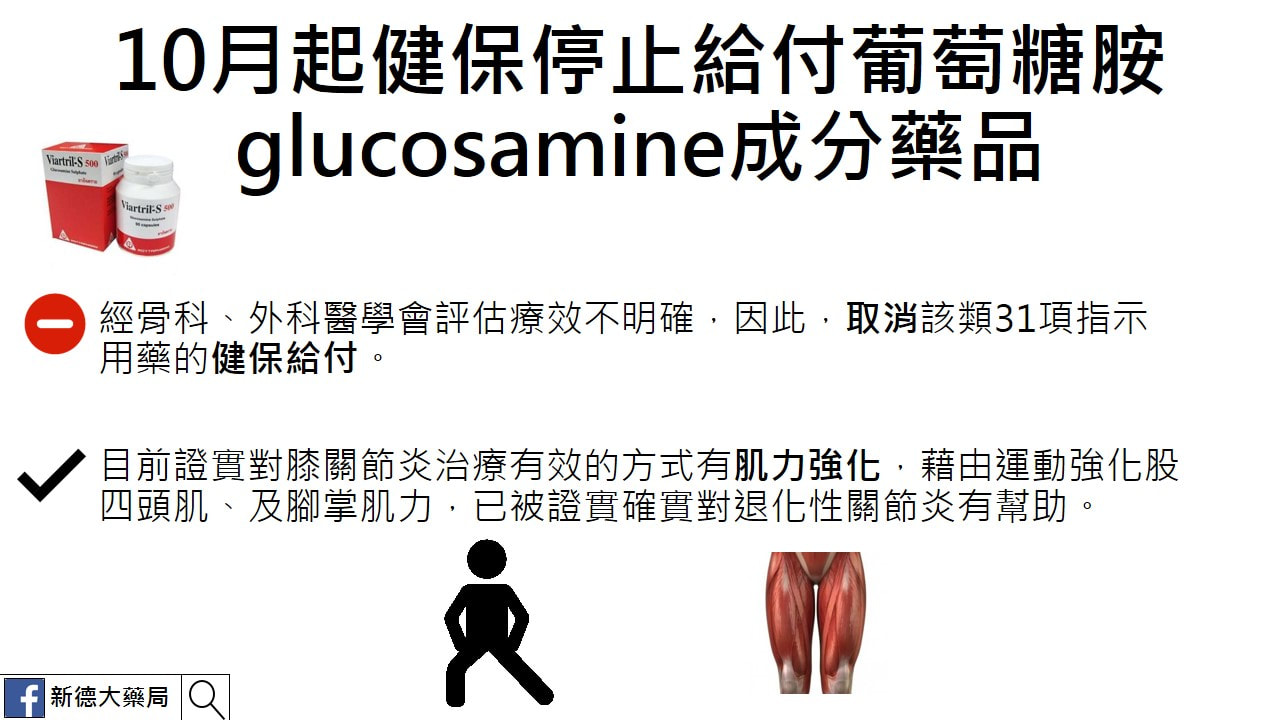 中華民國醫師公會全聯會去年底發函健保署,要求取消給付「維骨力」等含葡萄糖胺的31項指示用藥,經骨科、外科醫學會評估療效不明確,之後於去年的健保署共同擬訂會議中達成決議,確定取消該類31項指示用藥的健保給付,健保署今表示,經衛福部審查的最新結果,確定10月起取消這類藥品的健保給付,初估將影響12萬人,年省1.2億元健保支出。
健保署醫審及藥材組組長戴雪詠表示,健保署已將去年底健保署共同擬訂會議將「維骨力」等共31項含有葡萄糖胺的指示用藥停止健保給付的決議,送衛福部審查,近日獲得衛福部許可,因此已在8月23日發出公文,通知各醫學會及醫療院所,於今年10月起,即停止該項藥品的健保給付。 健保署醫審及藥材組專委黃兆杰表示,根據健保署最新統計今年1月至6月全台約有12萬人有在使用含葡萄糖胺glucosamine成分藥品,花費約6000萬元,自10月起健保停止給付後,初估將影響12萬人,年省1.2億元健保支出。 黃兆杰表示,指示藥不需經醫師處方民眾可自行到藥局購買,根據《健保法》指示用藥其實不應以健保給付,目前除了已確定停止給付的葡萄糖胺類藥物,仍有900多項指示用藥仍在給付中,過去停掉的已有1500多項藥物,健保署也將與各醫學會討論,並評估影響人數最少的指示用藥來停止健保給付。 長庚體系運動醫學委員會嘉義召集人許宏志表示,膝蓋軟骨是由一層網狀組織與網中的球狀組織所組成,網狀組織主要成分為二型膠原蛋白,網子內的球狀組織「蛋白醣」,則是由玻尿酸、葡萄糖胺、軟骨素所組成,因此早期治療退化性關節炎,除了使用抗發炎藥物,也會使用葡萄糖胺作為治療藥物。 但由於口服葡萄糖胺牽涉到每個人的劑量不一、吃下去不一定會直接補充到膝蓋、以及有可能不是軟骨,而是大腿、小腿骨鬆造成的膝蓋磨損,過去也有國外研究證實,一天750毫克的劑量其實對治療退化性關節炎並無顯著效果,因此現在認為應視葡萄糖胺為營養補充品而非治療藥物;傳統的單一類固醇藥物,也被實驗證實對治療退化性關節炎無明顯療效。 目前被證實對膝關節炎治療有效的方式有肌力強化,藉由運動強化股四頭肌、及腳掌肌力,已被證實確實對退化性關節炎有幫助;另外,葡萄糖及PRP增生治療注射,是這十幾年來才剛起步的新療法也被認為有治療潛力,但相關實證研究目前仍在進行中。(黃仲丘/台北報導) 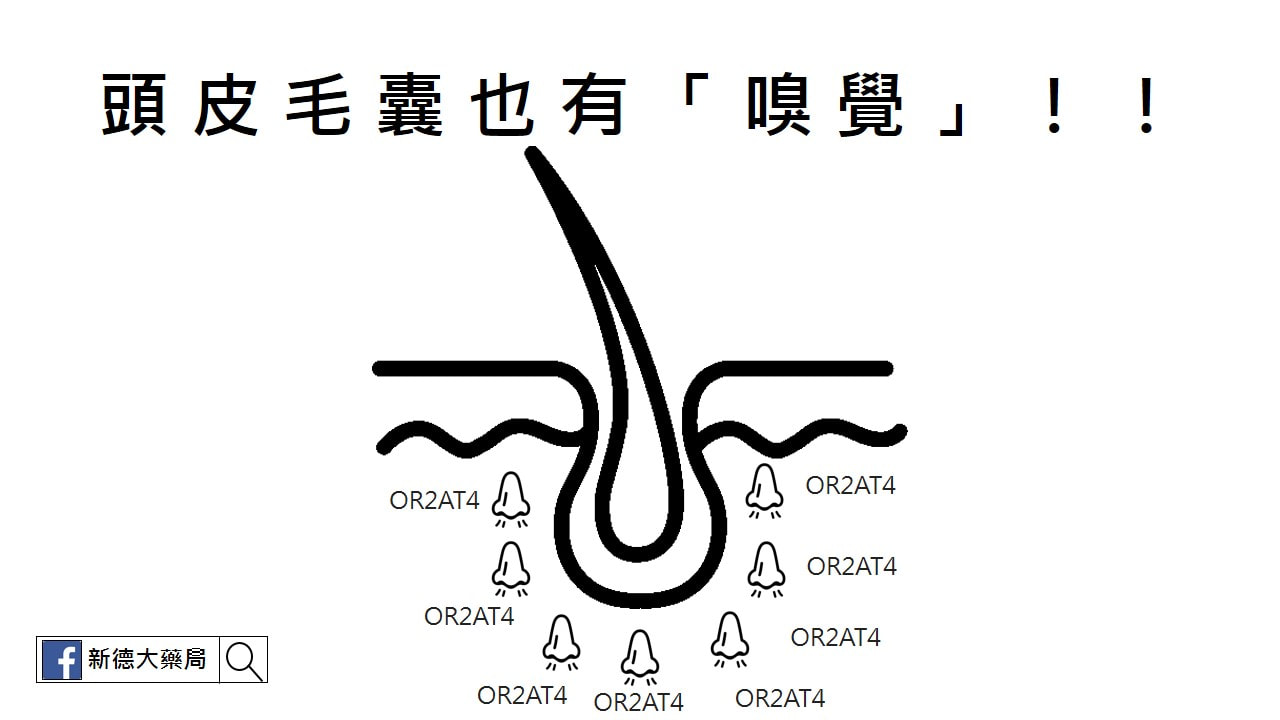 除了鼻腔裡的嗅覺細胞,近期一項國際知名NATURE的人體外試驗研究發現,頭皮毛囊也有「嗅覺」,若接受到特定香味的刺激,甚至能促使毛髮生長! Published: 18 September 2018 Olfactory receptor OR2AT4 regulates human hair growth 國曼徹斯特大學聯合美國、德國學者的研究指出一項驚人發現,人類毛囊細胞也有被稱為「OR2AT4」的嗅覺受體,可以聞到不同的氣味(結合氣味的化學分子,向大腦發出電子信號)。科學家至少發現了一種味道能刺激毛髮生長──這種味道正是常在芳香劑裡見到的「人工合成檀香味」。 研究團隊領導人,曼徹斯特大學的高級研究員兼皮膚科醫師Ralf Paus表示,「有史以來第一次證明,可以通過一種聞起來優雅又廣泛使用的芳香劑,來促進人體毛髮的生長。」 為了進行這個實驗,研究人員用了整形手術的患者捐贈的頭皮樣本,在實驗環境下使用人工合成檀香Sandalore刺激這塊頭皮,隨後毛囊細胞中一種「種類胰島素生長因子IGF-1」分泌提高,而這種激素能促進毛髮生長。 將另一種聞起來帶有花香甜味的人工香味劑Phenirat與毛囊細胞接觸後,IGF-1的分泌反而產生了抑制。這說明毛囊擁有自己「喜歡與否」的氣味,而反應在毛髮生長的情況上。 目前研究團隊認為用香味治療禿頭的方式大有可為,明年一月將啟動大型人體臨床實驗。 在沒有證實之前,建議還是先使用正規的醫療方式,需要使用外用生髮液(落建)或是口服用藥(柔沛或是新髮靈),都還是得照原來的方式。 千萬不要因為這個新聞,就停止用藥,改買人工合成檀香味的芳香劑來薰頭皮毛囊,萬一方法有誤,可能導致更嚴重的落髮喔! AbstractOlfactory receptors are expressed by different cell types throughout the body and regulate physiological cell functions beyond olfaction. In particular, the olfactory receptor OR2AT4 has been shown to stimulate keratinocyte proliferation in the skin. Here, we show that the epithelium of human hair follicles, particularly the outer root sheath, expresses OR2AT4, and that specific stimulation of OR2AT4 by a synthetic sandalwood odorant (Sandalore®) prolongs human hair growth ex vivo by decreasing apoptosis and increasing production of the anagen-prolonging growth factor IGF-1. In contrast, co-administration of the specific OR2AT4 antagonist Phenirat® and silencing of OR2AT4 inhibit hair growth. Together, our study identifies that human hair follicles can engage in olfactory receptor-dependent chemosensation and require OR2AT4-mediated signaling to sustain their growth, suggesting that olfactory receptors may serve as a target in hair loss therapy.
IntroductionOlfactory receptors (ORs) are part of an evolutionarily ancient chemosensory signaling system that long predates the development of smell sensation (olfaction)1,2,3,4,5,6,7. OR expression is not restricted to the nasal epithelium, but it is also present in several other human tissues8,9,10,11,12,13,14,15. Non-olfactory roles of ORs have also been described in human cell physiology16, such as in spermatozoa10,17 and enterochromaffin cells of the gut18. Interestingly, several ORs are also expressed in human epidermis19,20, including OR2AT4, whose selective activation by the synthetic sandalwood odorant (Sandalore®) promotes human epidermal keratinocyte migration and proliferation in vitro and wound re-epithelialization ex vivo20. Sandalore®-induced Ca2+ signaling could be blocked in OR2AT4-transfected Hana3A cells when this was co-applied at equimolar concentrations with the potent competitive OR2AT4 antagonist in presence of Sandalore®, Phenirat®20. Given the intimate connections between hair growth and wound healing21,22,23,24, we hypothesized that this OR might also impact on human hair growth. This hypothesis was investigated by immunohistology, qRT-PCR, western blot, microarray, phospho-kinase assay, and gene silencing in healthy, organ-cultured human scalp hair follicles (HFs)25. The present study shows that human HFs express a specific OR, namely, OR2AT4. The activation of this OR by its specific agonist, Sandalore®, prolongs anagen maintenance ex vivo by decreasing hair matrix keratinocytes apoptosis and increasing the production of IGF-1 in the outer root sheath (ORS). The anagen-prolonging effect mediated by Sandalore® is OR2AT4 dependent, as confirmed by co-administration of Sandalore® with the OR2AT4 competitive antagonist, Phenirat®, as well as the specific knock-down of OR2AT4 in human HFs. Taken together, we show that human HFs can engage in chemosensation and that the specific activation of OR2AT4 is required to sustain HF growth. ResultsHuman HFs express OR2AT4Immunofluorescence microscopy, qRT-PCR, and western blot analysis revealed that human scalp HFs in the anagen VI stage of the hair cycle26,27 express OR2AT4 at the transcript and protein level (Figs. 1a, 2a–f). Interestingly, OR2AT4 protein was predominantly expressed by suprabulbar keratinocytes of the proximal ORS (Figs. 1a, 2c), while hair matrix keratinocytes also expressed low-level OR2AT4 protein (Figs. 1a, 2b), both in healthy scalp skin in situ27 (Fig. 2a–c) and in amputated microdissected anagen HFs ex vivo25,26 (Fig. 1a). Of note, OR2AT4 expression was downregulated during spontaneous, apoptosis-driven HF regression (catagen)26,27 (Fig. 2d–g). Thus, using the primary antibody employed here20, intrafollicular OR2AT4 expression is strikingly restricted to defined epithelial HF compartments and is hair cycle dependent. Fig. 1 Hair follicles express OR2AT4, which specific stimulation endorses IGF-1-dependent anagen prolongation. a Representative images showing OR2AT4 protein expression (using the previously published OR2AT4 antibody20) in proximal outer root sheath and hair matrix keratinocytes of human scalp microdissected hair follicles. b Hair cycle score and staging were evaluated in treated and vehicle HFs after 6 days of culture using Ki-67/TUNEL immunofluorescence and Masson–Fontana histochemistry26. Mean ± SEM, n = 16–24 HFs from three donors (independent experiments), Kruskal–Wallis test (P = 0.0923, n.s not significant) and Dunn’s multiple comparisons test as post hoc test, ns not significant, Mann–Whitney test, *P < 0.05. Representative pictures of Masson–Fontana histochemistry in vehicle and treated HFs after 6 days of treatment. c Apoptotic hair matrix keratinocytes were counted in the hair matrix of all treated and vehicle HFs. Representative pictures of Ki67/TUNEL. Mean ± SEM, n = 18–21 HFs from three donors (independent experiments), Kruskal–Wallis (P = 0.005) test and Dunn’s multiple comparisons test as post hoc test, #P < 0.05, ##P < 0.01, ###P < 0.001. d IGF-1 expression was measured in ORS keratinocytes in treated and vehicle HFs. Representative pictures of IGF-1 immunofluorescence. IGF-1 expression was quantified in ORS keratinocytes in treated and vehicle HFs using ImageJ. Mean ± SEM, n = 18–21 HFs from three donors (independent experiments), Kruskal–Wallis (P < 0.001) and Dunn’s multiple comparisons test as post hoc test, ##P < 0.01, ###P < 0.001, and Student’s t-test, *P < 0.05. e Hair cycle score and staging were measured in treated and vehicle HFs after 6 days of culture. Representative pictures of vehicle and treated HFs after 6 days of treatment. Mean ± SEM, n = 22–29 HFs from three donors (independent experiments), Kruskal–Wallis test (P = 0.1434) and Dunn’s multiple comparisons test as post hoc test, n.s not significant, and Student’s t-test after performing an iterative Grubbs outlier test, *P < 0.05. CTS connective tissue sheath, DP dermal papilla, HM hair matrix, ORS outer root sheath, IRS inner root sheath, HS hair shaft. Scale bar: 100 µm Full size image Fig. 2 OR2AT4 mRNA and protein expression in human scalp epidermis and hair follicles in situ. aRepresentative pictures of OR2AT4 immunofluorescence in human scalp epidermis of three different donors (positive control20). Red line delineates the dermo-epidermal basement membrane. Cytosolic expression of OR2AT4 in hair matrix and suprabulbar outer root sheath (ORS) keratinocytes. Scale bar: 100 µm. b, c Representative pictures of confocal imaging of OR2AT4 immunofluorescence in human scalp HFs from three different donors (independent experiments). Scale bar: 100 µm. d, e mRNA (normalized against GAPDH) and in situ protein expression of OR2AT4 in anagen and catagen microdissected HF epithelium. Mean ± SEM, n = 3 from nine HFs/donor from three donors (independent experiments), Student’s t-test, *P < 0.05. f, g Western blot analysis and quantitative results of OR2AT4 (normalized against actin) in anagen and catagen microdissected human scalp HFs. Mean ± SEM from nine HFs/donor from two donors (independent experiments). The specific band for OR2AT4 is found around 44 kDa, although the predicted molecular weight of OR2AT4 is 36 kDa. This slight difference can be explained by a post-translational modification (an acetylation site has been identified on the lysine at the position 303 [source: phosphoSitePlus®]) that would increase the molecular weight64. A1-2 indicates anagen HFs and C1-2 indicates catagen HFs from donor 1 and 2. DP dermal papilla, HM hair matrix Full size imageOR2AT4 activation by Sandalore® prolongs anagen ex vivoWhen microdissected, organ-cultured human HFs25 were treated with Sandalore® (500 μM, for details, see Supplementary Note 1 and Fig. 3a–e) for 6 days, this selective OR2AT4 agonist20 significantly upregulated intrafollicular OR2AT4 protein expression (Fig. 3d), demonstrating receptor functionality and that OR2AT4 expression underlies a positive feedback regulation. Fig. 3 High concentration of Sandalore® (500 µM) regulates hair matrix keratinocytes apoptosis and intrafollicular OR2AT4 expression. a, b The number of Ki-67+ and TUNEL+ cells in the hair matrix was evaluated in the hair bulb of all treated and vehicle HFs. c Representative pictures of Ki-67/TUNEL staining. Mean ± SEM, n = 19–21 HFs from two donors (independent experiments), unpaired Student’s t-test or Mann–Whitney test, *P < 0.05, **P < 0.01. DP dermal papilla, HM hair matrix. Scale bar: 100 µm. d OR2AT4 protein expression was evaluated using ImageJ in the ORS of Sandalore®-treated and control HFs after 6 days of culture. e Representative pictures of OR2AT4 expression in the ORS of cultured HFs. Mean ± SEM, n = 12–15 HFs from two donors (independent experiments), Student’s t-test, *P < 0.05. CTS connective tissue sheath, IRS inner root sheath, ORS outer root sheath. Scale bar: 100 µm Full size imageImportantly, Sandalore® treatment retarded spontaneous HF regression (catagen development)26,27 ex vivo (Fig. 1b) and significantly reduced hair matrix keratinocyte apoptosis, as shown by quantitative (immuno-)histomorphometry for TUNEL+ (Fig. 1c) or cleaved caspase 3+ cells (Supplementary Fig. 1a) in the hair matrix. These effects were partially counteracted by co-administering the competitive OR2AT4 antagonist, Phenirat®20, with Sandalore® (Fig. 1b, c, Supplementary Fig. 1a). When tested alone, Phenirat® tended to be weakly hair growth inhibitory (Supplementary Fig. 2a, b and Supplementary Note 2 for extended discussion). Next, we examined two key growth factors that control the anagen-catagen transformation during human HF cycling, i.e., catagen-promoting TGF-β2 and anagen-maintaining IGF-1; these growth factors are prominently produced by those proximal ORS keratinocytes28,29,30,31,32,33 that express OR2AT4 maximally. This analysis revealed a significant decrease in TGF-β2 (Supplementary Fig. 3a) and a significant increase of IGF-1 (Fig. 1d) protein expression in the proximal ORS after long-term Sandalore® treatment ex vivo. The co-administration of OR2AT4 antagonist, Phenirat®, significantly reversed the Sandalore®-induced intrafollicular upregulation of IGF-1 (Fig. 1d) but did not affect TGF-β2 expression (Supplementary Fig. 3a). Anagen-prolonging effect of Sandalore® is OR2AT4 specificSubsequently, we selectively silenced OR2AT4 by siRNA administration to organ-cultured human scalp HFs ex vivo32,34,35, as documented by significantly reduced intrafollicular OR2AT4 mRNA and protein expression (Fig. 4a, b). Despite the presence of excess ligand (Sandalore®), OR2AT4 knock-down significantly promoted catagen induction compared to HFs treated with scrambled oligos (Fig. 5a), decreased IGF-1 protein expression (Fig. 5b), and enhanced hair matrix keratinocyte apoptosis (Fig. 5d, e). Instead, hair matrix keratinocyte proliferation (Fig. 5c) or TGFβ2 protein expression in the ORS (Supplementary Fig. 4a) remained unaffected. These data show that the Sandalore®-induced hair growth stimulation documented above is indeed OR2AT4 dependent, rather than due to off-target effects of this synthetic odorant and that OR2AT4 signaling is required for anagen maintenance. Fig. 4 OR2AT4 expression in Scambled oligos or siRNA OR2AT4 Sandalore®-treated, microdissected human scalp HFs after 6 h of organ culture. a Microdissected, human scalp HFs were treated for 6 h with OR2AT4 siRNA or scrambled oligos, using the intrafollicular gene silencing technique32. OR2AT4 mRNA expression was evaluated after 24 h of culture in siRNA or scrambled oligo-transfected HFs. b OR2AT4 protein expression was evaluated using ImageJ in the ORS of siRNA-treated and control HFs after 6 days of culture. Representative pictures of OR2AT4 expression in the ORS of cultured HFs. Mean ± SEM, n = 19–24 HFs from three donors (independent experiments), Student’s t-test, *P < 0.05, ***P < 0.001. CTS connective tissue sheath, IRS inner root sheath, ORS outer root sheath. Scale bar: 100 µm Full size image Fig. 5 The anagen prolongation effect of Sandalore® is OR2AT4 dependent. a Hair follicle cycle score and staging were performed in HFs treated with siRNA OR2AT4 or scrambled oligos in the presence of Sandalore®32. Representative images of vehicle and treated HFs after 6 days of treatment. Mean ± SEM, n = 16–18 HFs from three donors (independent experiments), Mann–Whitney test, *P < 0.05. b IGF-1 expression was quantified in ORS keratinocytes in treated and vehicle HFs using ImageJ. Representative pictures of IGF-1 immunofluorescence. Mean ± SEM, n = 22–24 HFs from three donors (independent experiments), Mann–Whitney test, *P < 0.05. c, d Ki67+ cells and TUNEL+ cells were counted in the hair matrix of siRNA and control HFs. Representative pictures of Ki67/TUNEL double-staining in the hair bulb of HFs. Mean ± SEM, n = 17–18 HFs from three donors (independent experiments), Mann–Whitney test, *P < 0.05, n.s. not significant. e The number of cleaved caspase-3+ cells (white arrows) in the hair matrix was evaluated in the hair bulb of all HFs treated with OR2AT4-siRNA or scrambled oligos. Representative pictures of cleaved caspase-3 staining. Mean ± SEM, n = 18 HFs from three donors (independent experiments), Student’s t-test, *P < 0.05. CTS connective tissue sheath, DP dermal papilla, HM hair matrix, ORS outer root sheath, IRS inner root sheath. Scale bar: 100 µm Full size imageSandalore®-mediated HF response involves different pathwaysMicroarray analysis independently confirmed anti-apoptotic effects of Sandalore® (Fig. 6, Supplementary Fig. 5, and Supplementary Data 1), since transcripts of pro-apoptotic genes were significantly downregulated (e.g., TP53AIP1: -10.27×), while anti-apoptotic genes were significantly upregulated (e.g., FGF-2: +7.83×) in HFs treated short term with Sandalore® (6 h, Supplementary Fig. 5a, b and Supplementary Data 1). Interestingly, an additional microarray analysis of organ-cultured scalp HFs in which OR2AT4 had been knocked down ex vivo showed that transcription of the IFI6 (G1P3) gene, whose silencing increases keratinocyte apoptosis36, was downregulated by administering OR2AT4 siRNA for 6 h, compared to scrambled oligonucleotide-treated HFs (Supplementary Fig. 6a, b and Supplementary Data 1). This corresponds well to our observation that OR2AT4 silencing increases apoptosis of HF matrix keratinocytes (Fig. 5d, e) and further underscores the importance of continued OR2AT4 stimulation by as yet unknown endogenous ligands to suppress apoptosis in the hair matrix of human anagen HFs. Fig. 6 Microarray-based analysis of genes related to anagen-prolonging pathways after stimulation with Sandalore® (500 µM). a, b Venny diagrams65 show the upregulated and downregulated genes (cut-off: fold change >−1.8 or >+1.8 and equidirectional changes). White squares indicate genes upregulated and downregulated in at least three of four donors (independent experiments). The heatmap shows the list and the expression level of the most upregulated and downregulated genes related to the different pathways regulated after OR2AT4 activation (cut-off: fold change >−1.8 or >+1.8 and equidirectional changes) in at least three of four donors (independent experiments) (c). Green: apoptosis related, orange: dermcidin related, and violet: IGF related Full size imageIn addition, microarray analysis revealed that Sandalore® promotes signaling along the IGF pathway (see Fig. 6a–c, Supplementary Fig. 5a-b, and Supplementary Data 1), in agreement with the protein expression data (Fig. 1d). Indeed, genes involved in IGF1R signaling cascade as well as in IGF transport (e.g., PAPPA [10.8× upregulated] that cleaves IGFBP4 to release IGF37, or PCSK-1 [33.6× upregulated] which is involved in insulin synthesis from proinsulin38) were strongly upregulated (Fig. 6a–c, Supplementary Fig. 5, and Supplementary Data 1). This promotion of IGF signaling pathway as well as the upregulation of FGF-7 (2.75× increase), another anagen-promoting growth factor39 (Fig. 6a–c, Supplementary Fig. 5, and Supplementary Data 1) are perfectly in line with anagen prolongation by Sandalore®. Intriguingly, the strongest transcriptional upregulation (77.6× increase) was seen for dermcidin, a potent antimicrobial peptide with broad bactericidal activities that reportedly is only produced by sweat gland epithelium in human skin40,41. However, quantitative immunohistomorphometry confirmed that dermcidin protein is also upregulated by Sandalore® in the epithelium of human scalp HFs (Supplementary Fig. 7a and Table 1). This demonstrates that human HFs also express dermcidin and raises the fascinating question whether OR2AT4 may act as a chemosensory receptor for selected bacterial metabolites, in response to which intrafollicular dermcidin production may be upregulated to manage the complex HF-microbiome42,43. Table 1 OR2AT4 stimulation by Sandalore®treatment regulates different signaling protein phosphorylation pathways in human HFs ex vivo Full size tableWhen selected signaling pathways recognized to be involved in OR-mediated signaling1,9,44,45,46,47, were studied by phospho-kinase assay9, Sandalore® upregulated several expected kinase activities (Fig. 7a and Table 1). In line with our previous results (Fig. 1c, d), this included increased phosphorylation of proline-rich AKT1 substrate 40 (PRAS40), whose expression is induced by IGF-148,49, while Sandalore® reduced phosphorylation of p53 (S46), which is highly phosphorylated in apoptotic cells50 (IGF-1 is a key apoptosis suppressor51,52,53). Fig. 7 OR2AT4 stimulation by Sandalore® treatment regulates different protein phosphorylation signaling pathways in human HFs ex vivo. Plot showing regulation of the phosphorylation of 45 kinases mediated by Sandalore® (50 and 500 µM) in cultured microdissected HFs from four different donors (independent experiments). Among those kinases, the most interesting ones underline in green (upregulated) and red (downregulated) rectangles. PRAS40 proline-rich AKT1 substrate 4049, S46 phosphorylated p5350, p53 phosphoprotein p53, p38α mitogen-activated protein kinases 14, ERK1/2 extracellular signal-regulated kinases1/2, EGFR epidermal growth factor receptor, MSK1/2 mitogen- and stress-activated protein kinase 1/2, PYK2 protein tyrosine kinase 2, Hsp60 heat shock protein 60, JNK1/2/3 c-Jun N-Terminal Protein Kinase 1/2/3, AMPKα1 AMP-activated protein kinase α1, PLCγ phospholipase C γ1, Fgr Feline Gardner-Rasheed proto-oncogene, WNK1 WNK lysine-deficient protein kinase 1 isoform Full size imageAnagen-prolonging effect of Sandalore® implicates IGF-1Therefore, we next probed the hypothesis that, mechanistically, Sandalore® stimulation of OR2AT4 may retard catagen and suppress HF apoptosis by upregulating intrafollicular IGF-1-mediated signaling. Indeed, the co-administration of IGF1-neutralizing antibody with Sandalore® significantly reversed the catagen-promoting effect of IGF-1 neutralizing antibody alone (Fig. 1e; for extended discussion, see Supplementary Note 3). Mechanistically, this suggests that OR2AT4 activation mainly prolongs anagen via upregulating IGF-1 expression and secretion by OR2AT4+ keratinocytes in the proximal ORS (Figs. 1d, 8). While IGF-1 signaling is known to be involved in olfactory bulb development and function54,55,56, the current study reveals that IGF-1 expression/secretion in human epithelial tissue is also controlled by OR-mediated signaling and demonstrates that IGF-1 production underlies an OR2AT4-controlled chemosensory regulation. Fig. 8 Proposed mechanism of action of OR2AT4 activation by Sandalore® and (unknown) endogenous ligand(s) in human hair follicle epithelium. The activation of OR2AT4 at the cell surface of outer root sheath keratinocytes (ORS KCs; location: see green cells in the central HF cartoon) by endogenous ligands and/or Sandalore® upregulates the expression of genes and kinases involved in programmed cell death, thus preventing intrafollicular apoptosis (e.g., by phosphorylation of PRAS40 preventing its interaction with mTOR1, upregulation of NF-κB pathway) or downregulates key players in the apoptotic machinery (e.g., dephosphorylation of p53, downregulation of Bad). In parallel, OR2AT4 activation by exogenous (Sandalore®) or endogenous ligands (e.g., metabolites of the HF microbiome) induces the upregulation of PAPPA that cleave the IGFBP4/IGF1 complex to release IGF-1 (pink arrows). The released IGF-1 triggers the activation of IGF-1R on the same cell (autocrine signaling, purple arrow) or on hair matrix keratinocytes (HM KCs; orange “cell”) (paracrine signaling, orange arrow). The activation of IGF-Rs on HM keratinocytes then induces signaling cascades (e.g., PI3K/AKT and/or p38a/ERK1/2/MSK1/2) that activate different transcription factors and particularly CREB, which results in an anti-apoptotic effect and prolonged anagen phase in human HFs. P phosphorylation, green square gene upregulation, red square gene downregulation, green circle phosphorylation, red circle dephosphorylation Full size imageDiscussionCollectively, these data show that the growth, cyclic transformation, epithelial cell apoptosis, and IGF-1 production of a dynamic human (mini-)organ, i.e., scalp HFs29, underlies an OR-dependent chemosensory control. Thus, human HFs can “smell” in the sense that they recruit the evolutionarily oldest and largest of all receptor families1,2 for regulating key organ functions (for extended discussion, see Supplementary Discussion 1). Moreover, we identify one specific OR, namely, OR2AT4, whose stimulation with a synthetic agonist (Sandalore®)20 and whose selective silencing profoundly impacts on human hair growth ex vivo primarily via regulating expression and secretion of the key hair growth-promoting factor, IGF-1 (Fig. 8 and Supplementary Discussion 2). However, while IGF-1-mediated signaling is required for human hair growth promotion by Sandalore® (Fig. 1e), our phospho-kinase activity and gene expression profiling results suggest that additional pathways (e.g., p38a/ERK1/2/MSK1/2, HB-EGF/EGF-R, and FGF-7 pathways (Fig. 6, Supplementary Figs. 5, 6, and Supplementary Data 1)) are involved that deserve further exploration57,58,59,60,61. Perhaps most intriguingly, our silencing data suggest that OR2AT4-mediated signaling is required for maintaining human scalp HFs in anagen and for suppressing keratinocyte apoptosis in the hair matrix (Fig. 5d, e). This begs the question: What are the endogenous intrafollicular OR2AT4 ligands in human HFs? The endogenous ligands for human ORs remain to be definitively clarified, and those for OR2AT4 are unknown. Candidates include molecules with Sandalore®-like structure, short-chain fatty acids13, and—namely, in view of our dermcidin results (Supplementary Fig. 7a and Table 1)—metabolites of resident HF microbiota42,43. Taken together, our ex vivo data suggest that olfactotherapy by topically applied cosmetic OR2AT4 ligands like Sandalore® may promote human hair growth by prolonging anagen and inhibiting premature catagen development (e.g., in androgenetic alopecia and telogen effluvium). Thus, using scalp HFs as accessible and tractable model organs and by selectively targeting OR2AT4, our study reveals an important, translationally relevant frontier in the OR-dependent chemosensory physiology of peripheral human tissues. MethodsHuman samplesTemporal and occipital human scalp skin was obtained from healthy donors (38–69 years old) undergoing routine face-lift surgery after informed consent and ethical approval (University of Muenster, no. 2015-602-f-S). No sample size calculation was performed. Number of three different donors was used due to the small availability of the tissue used in the study. This number of three was used in many previous studies, given statistical significance. Tissue specimensScalp skin samples were either cut into small pieces (4 mm), embedded into OCT, and frozen in liquid nitrogen, or processed for HF microdissection25. HF organ cultureHuman scalp samples were obtained 1 day after face-lifting procedure (i.e., after overnight transport from collaborating surgeons) and used at the same day for microdissecting human anagen VI scalp HFs. The HF microdissection technique employed for setting up the classical Philpott assay25,26,62 used in the current study, removes all perifollicular tissue with the sole exception of the HF’s dermal sheath, and thus does not contain any other skin appendage structures (e.g., eccrine gland elements)25. Microdissected human scalp HFs were cultured at 37 °C with 5% CO2 in a minimal media of William’s E media (WEM, Gibco, Life Technologies) supplemented with 2 mM of L-glutamine (Gibco), 10 ng/ml hydrocortisone (Sigma-Aldrich), 10 μg/ml insulin (Sigma-Aldrich), and 1% penicillin/streptomycin mix (Gibco)25,26,62. After microdissection, the HFs were first incubated in WEM for 24 h for re-equilibration. HFs after quality control (fully pigmented and presence in anagen VI phase) were randomly allocated to the different experimental groups. Chemical stimulation of human microdissected HFsAfter 24 h, WEM medium was replaced and HFs were treated with vehicle (0.1% DMSO), Sandalore® (50 and 500 µM; see Fig. 3 and Supplementary Note 1, Symrise), Phenirat® (in a ratio 1:1 to the agonist, Symrise), or Sandalore®+Phenirat® for 6 days for (immuno-)histology or 6 h for qRT-PCR. For the IGF-1 neutralizing antibody experiments, IGF-1 neutralizing antibody (1 µg/ml, ab9572, Abcam) was added 30 min before adding Sandalore® to the corresponding groups. Culture medium was replaced every second day and after 6 days. HFs were then embedded in cryomatrix (Fisher Scientific), and snap frozen in liquid nitrogen for (immuno-)histology. SiRNA transfection-knockdown OR2AT4 in organ-cultured HFsHuman anagen VI HFs were transfected using a commercial siRNA reagent system (Sc-45064, Santa Cruz) following the manufacturer’s instructions32,34,35. Briefly, stock solutions (10 µM) of siRNA OR2AT4 (gift from Prof. Hanns Hatt20) and siRNA control (scrambled oligo) were prepared using RNAse-free water. HF transfection was performed 24 h after microdissection for 6 h using either 100 mM OR2AT4 siRNA or control scramble siRNA. After 24 h of incubation with fresh WEM medium, HFs were collected per group in RNA later and stored at 4 °C for further RNA extraction and qRT-PCR analysis or immediately frozen in liquid nitrogen and stored at −80 °C for microarray analysis. Finally, fresh WEM medium was replaced every second day and after 5 days of culture, HFs were snap frozen in OCT for further quantitative (immuno-)histomorphometry analysis. HistologyFor histochemical visualization of melanin, Masson–Fontana staining was performed on frozen sections. Melanin was stained as brown dots26. ImmunofluorescenceOCT-embedded samples were sectioned (6 µm thickness for HF and 7 µm thickness for skin) with a Leica cryostat. For primary OR2AT420(custom designed rabbit polyclonal antibody generated against the C-terminus sequence of OR2AT4 (Eurogentec, Liège, Belgium)), or cleaved-caspase-3 (#9661, clone Asp175, Cell Signaling) antibodies staining, tissue cryosections were fixed in 4% paraformaldehyde, pre-incubated with 10% of goat serum (for OR2AT4) or 5% goat serum +0.3% Tritton X-100 (for cleaved-caspase 3) and incubated with the corresponding primary antibody at 4 °C overnight (1/100 for OR2AT4 and 1/400 for cleaved-caspase 3). Secondary antibody incubation was performed at RT for 45 min. Counterstaning with DAPI (1 µg/ml) was performed to visualize nuclei. Dermicidin protein was detected using tissue sections fixed in 4% paraformaldehyde, pre-incubated with 10% of goat serum, and incubated with a mouse anti-human Dermcidin antibody (Novus Biologicals, G-81, 1:200). Secondary antibody (Goat anti-mouse Alexa fluor 488) incubation was performed at room temperature for 45 min. Counterstaning with DAPI (1 µg/ml) was performed to visualize nuclei. For TGFβ2 (Sc-90, Santa Cruz) and IGF-1 (Sc-1422, clone G-17, Santa Cruz31,32), tissue cryosections were fixed in acetone and endogenous peroxidase activity was blocked with 3% of H2O2 (Merck Milipore). This step was followed by an avidin-biotin blocking step (SP2001, Vectorlabs) and a preincubation with TNB buffer (Tris HCl+NaCl+Casein). The corresponding primary antibody was incubated at 4 °C overnight (1/1000 for TGFβ2 and 1/250 for IGF-1). Secondary antibody incubation was performed at RT for 45 min before using the Tyramide signal amplification kit (NEL700001KT, Perkin Elmer). Counterstaning with DAPI was performed to visualize nuclei. To stain apoptotic and proliferating cells, we used the apoptag kit (Merck Milipore) following the manufacturer’s protocol followed by Ki-67 staining25,26,33,63. Primary antibody was incubated overnight (Ki-67, M7240 Clone: MIB-1, DAKO, 1/20) after the TdT-enzyme step. The secondary antibody was incubated for 45 min at RT after the fluorescent-labeled anti-Digoxigenin step of the apoptag kit. Counterstaning with DAPI was performed to visualize nuclei. Negative controls were performed by omitting the primary antibody. Images were taken using a Keyence fluorescence microscope BZ9100 (Osaka, Japan) maintaining a constant set exposure time throughout imaging for further analysis. Quantitative reverse transcriptase-PCRTotal RNA was isolated from whole microdissected HFs using RNeasy Mini Kit (Quiagen) following the manufacturer’s instructions described in the manufacturer’s protocol. RNA purity and concentrations were determined using the Nanodrop ND-1000 assay (Fisher Scientific). Reverse transcription of the RNA into cDNA was performed using the TetrocDNA Synthesis Kit (Bioline), according to the manufacturer’s instructions. RNA concentrations were adjusted between 50 to 500 nM for each sample set to allow further quantification comparison between samples and experiments after qRT-PCR. Controls were performed using the housekeeping gene GAPDH. Real-time quantitative polymerase chain reaction (qRT-PCR) was run in triplicate using TaqMan Fast Advanced Master Mix Product Insert and gene Expression Assay transcripts (Id: Hs01060665_g1 for ACTB, Hs02758991_g1 for GAPDH, and Hs02339277_s1 for OR2AT4, Applied Biosystem) on the qTower2.2 thermocycler. Real-time quantification plots and Ct values were collected and stored by the qPCRsoft2.1 software. The amount of the transcripts was normalized to those of the housekeeping gene using the ΔΔCT method using EXCEL. Whole-genome microarray analysisRNA isolation, sample processing, and microarray analyses (Agilent Technologies), as well as statistical evaluation, were performed by Arrows Biomedical GmbH (Muenster, Germany). Expressional alteration was considered to be significant only when ≥1.8-fold and equidirectional changes were observed in at least three of four patients (independent experiments). An additional analysis has been performed using 5-fold and equidirectional changes in the four different donors (independent experiments) in order to identify the top up and downregulated genes. Human phospho-kinase arrayIn order to gauge which signaling pathways are regulated by the specific stimulation of OR2AT4, we performed a phospho-kinase array9. Total protein was isolated from whole microdissected HFs using a specific buffer from the Human Phospho-Kinase Array (ARY003B, R&D System), following the manufacturer’s protocol. Briefly, protein extracts were diluted and incubated overnight with the Human Phospho-Kinase Array. The array was washed to remove unbound proteins, followed by incubation with a cocktail of biotinylated detection antibodies. Streptavidin-HRP and chemiluminescent detection reagents were applied, and a signal was produced at each capture spot corresponding to the amount of phosphorylated protein bound. Western blot analysisTotal protein was extracted from nine anagen and catagen microdissected human scalp HFs. Protein concentrations were determined using a Bradford assay (B6916, Sigma-Aldrich). Thirty micrograms of protein were subjected to 4–15% Mini-PROTEAN®TGX™ Precast gel (#4561083, Bio-Rad) and transferred to a nitrocellulose membrane (88018, Thermo Fisher Scientific), followed by incubation with the corresponding primary antibodies (PA5-71599 for OR2AT4, 1/1000, Thermo Fisher Scientific; and A3853 for Actin, 1/1000, Sigma-Aldrich) overnight at 4 °C. After incubation with peroxidase-conjugated secondary antibodies (WesternBreeze™ Chemiluminescent Kit, WB7106 and WB7104, Thermo Fisher Scientific), the bands were visualized using Chemocam imager 6.0 (Intas, Germany). Protein expression levels were normalized to corresponding actin levels. The uncropped blots are presented in the Supplementary Fig. 8. Hair cycle score (HCS) and stagingHFs were microscopically evaluated for the hair cycle staging analysis using Masson–Fontana histochemistry and Ki-67/TUNEL immunostainings25,26. The HCS was also measured25,31, which consists of assigning an arbitrary unit for each stage of the hair cycle (Anagen VI = 100; Early catagen = 200; Mid-catagen = 300; and Late catagen = 400). After having classified each HF according to its hair cycle stage, following the previously defined objective classification criteria for organ-cultured human HFs26, for each experimental condition, the mean HCS was calculated. The closer the mean is to 100, the higher is the number of anagen VI HFs in a given group. The HCS provides a global read-out parameter that looks at all HFs in a given experimental group and synthesizes them into a single number, which reflects how close the majority of HFs is to either anagen VI or catagen and also permits statistical analysis that it is not possible with hair cycle staging. Therefore, hair cycle staging and the HCS are independent read-out parameters that complement each other. Quantitative (immuno-)histomorphometryStaining intensity was evaluated in well-defined reference areas by quantitative (immuno-)histomorphometry 31,32, using NIH ImageJ software (NIH, Bethesda, MD, USA). Statistical analysesAll data are expressed as mean ± SEM (and variance is different between the groups) and were analyzed by one-way ANOVA or Kruskall–Wallis test and Dunn’s multiple comparisons test as post hoc test when more than two groups were compared or Student’s t-test or Mann–Whitney test when only two groups were compared (GraphPad Prism 6, GraphPad Software, San Diego, CA, USA) after performing d’Agostino and Pearson omnibus normality test. P < 0.05 was regarded as significant. 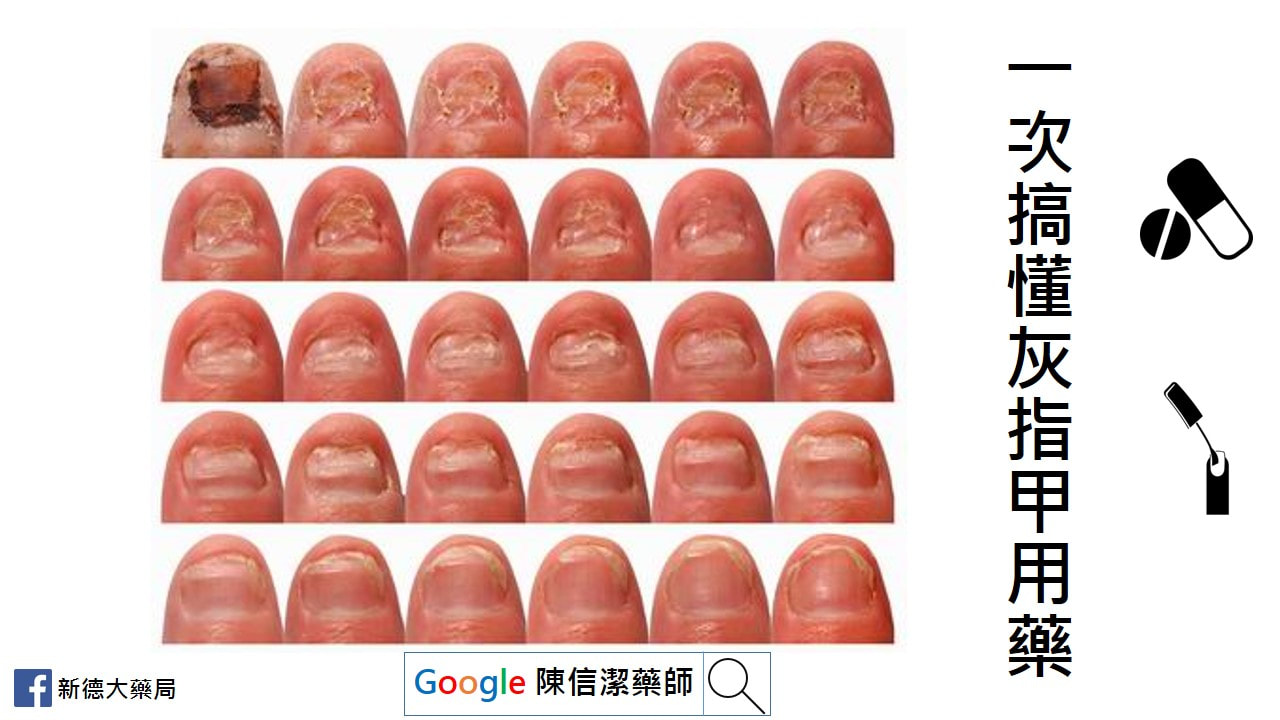 灰指甲就是指甲受黴菌感染,灰指甲常會併發在香港腳(足癬)患者身上。 正式的名稱叫『甲癬』。 台語稱『臭甲』。 哪些人容易感染灰指甲? 1、老年人 2、赤腳走在游泳池、健身房的淋浴間、公共浴池…等潮濕的表面 3、香港腳(足癬)患者 4、足部容易有小傷口,或是其他皮膚疾病,例如乾癬患者 5、糖尿病患者 6、各種免疫缺乏疾病患者 7、家中有其他人罹患灰指甲 灰指甲一定是灰色的嗎? 灰指甲常見的顏色有黃色、褐色、綠色等。 為什麼建議治療灰指甲? 嚴重者會有指甲增厚、周邊脫屑、指甲凹陷、指甲變形、甚至是甲床分離的情形。 有時會導致甲溝炎、凍甲、鉗甲等。 更嚴重者,還需要指甲矯正。 灰指甲合併香港腳會? 跟香港腳互相交錯感染,嚴重感染時,甚至偶會導致蜂窩性組織炎。 灰指甲會傳染嗎? 只要鞋子放在一起,或是一同出入潮濕地面,都很容易傳染。 例如:父母有灰指甲就很容易傳染給小孩。 治療灰指甲的方法有 1、傳統外用藥物 2、指甲油劑型藥物 3、口服藥物 4、指甲拔除術 5、雷射治療 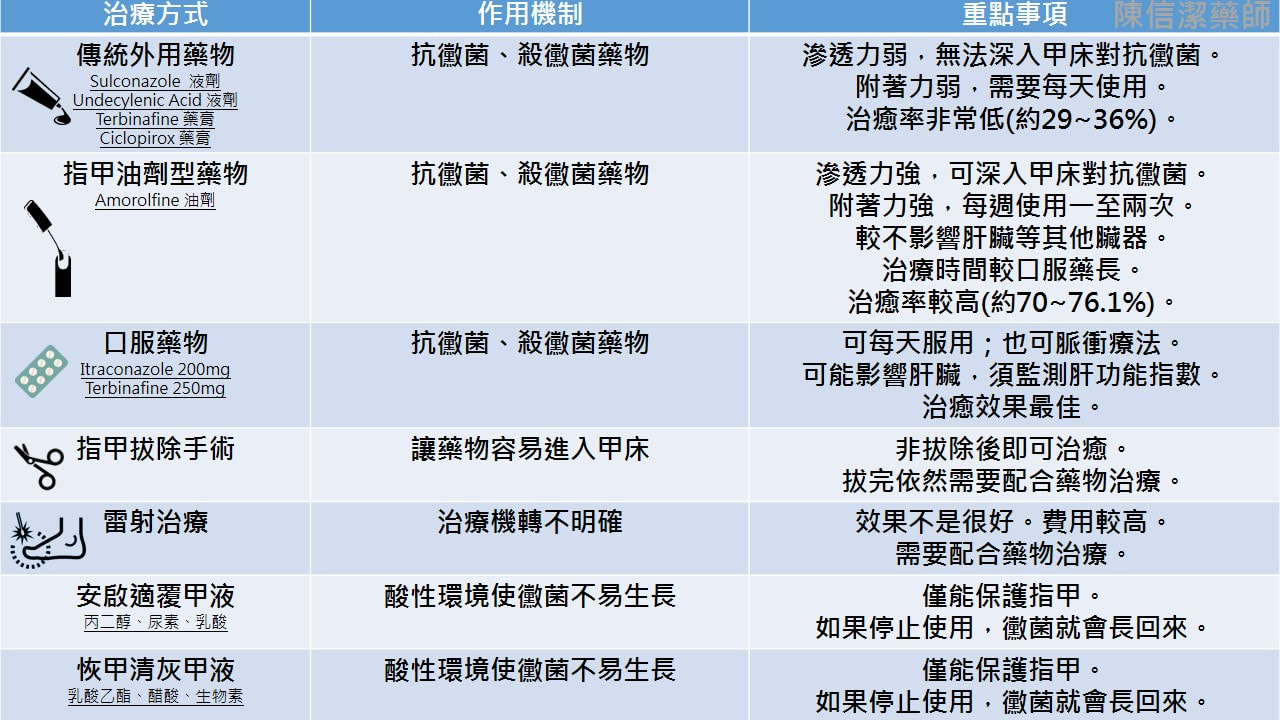 安啟適是甚麼呢? 在他們的官網上找到一篇關於此產品的研究文獻(JCDSA, Vol.1, No.3, 2011, pp.59-63),讓我們來一探究竟: 文獻中提到安啟適®覆甲液的成分為丙二醇、尿素和乳酸。 丙二醇是常見於化妝品中的成分,可做為乳化劑及防腐劑,美國FDA歸類為「大致認為安全食品」的食品添加物。 尿素通常在藥品或化妝品中用於保濕及去角質,幫助藥品吸收滲透。 乳酸也可用於軟化角質。 此三成分用於灰指甲的配方在一篇1989年的文獻中提出,因此可說是老藥新賣吧。 官網提供的文獻是在瑞典進行,收案75人,最終72人完成整個療程。值得一提的是,實驗中將近端甲下真菌病(proximal subungual onychomycosis,PSO)排除,也許是因為此類灰指甲較常是因糖尿病、愛滋病等其他疾病引起吧。 實驗在第2、4、8周各追蹤一次,最終第8周病人在四級自我評估結果大多落在中間「部分改善」(39.7%)與「明顯改善」(39.7%),8.2%的人認為「無感善」,12.3%認為「非常好的改善」。 「安啟適®覆甲液」算是一個老配方新產品,文獻的實驗規模不大,單就實驗結果來看,使用「安啟適®覆甲液」後8周多數患者感覺灰指甲狀況有改善,但完全治癒的比率並不高。以安全性而言此配方式算是安全且少有副作用的成分。 恢甲清又是什麼呢? 成分有乳酸乙酯(乳化劑及防腐劑)、 醋酸<獨家突破性滲透技術(TransActive™Technology)>沒有實驗證明,也沒有專利? 、生物素(提供指甲營養素....靠外用的吸收營養恐怕有點難度) 不論恢甲清或是安啟適在台灣此產品申請為醫材,效能是「限保護因真菌感染與創傷而受損的指甲」,和廣告中宣稱的改善灰指甲感染問題有微妙的差異..... 治療灰指甲還是要以正 藥物治療為主,至於恢甲清或是安啟適則是用來改善外觀,無法達到指甲上完全沒有黴菌的效果。因此如果停止使用,黴菌就又長回來。 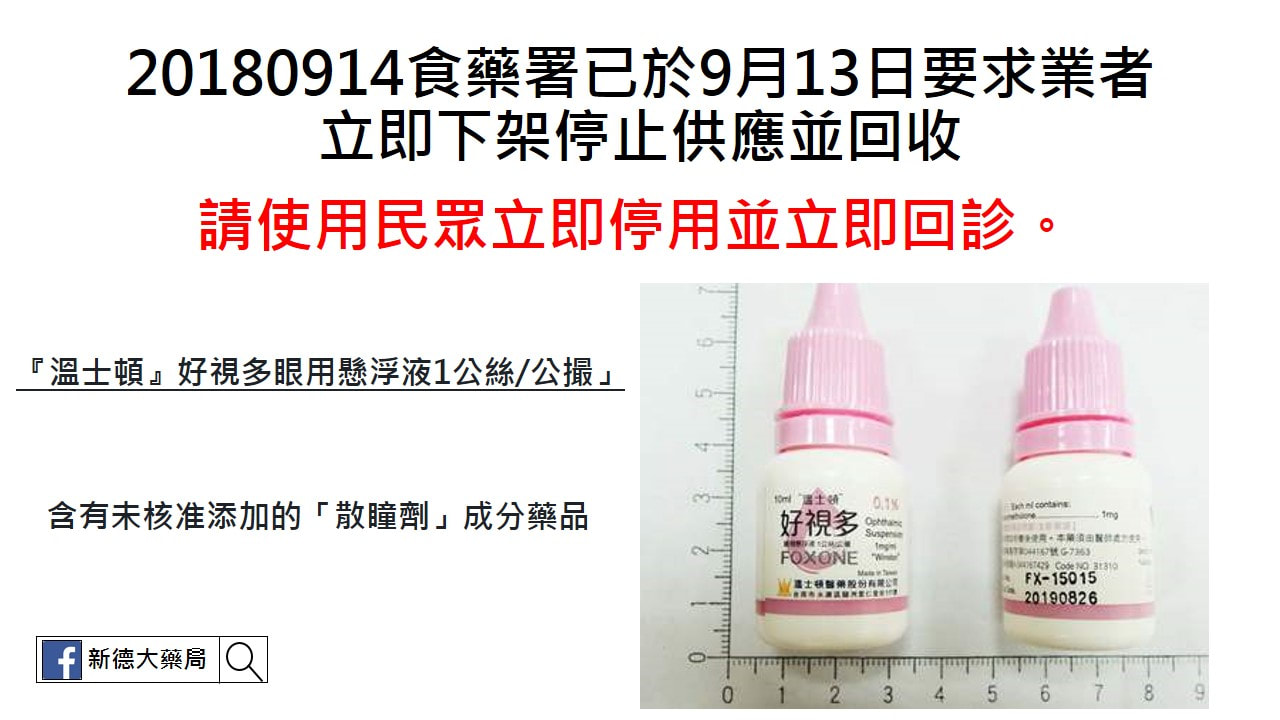 食品藥物管理署(下稱食藥署)檢出「"溫士頓" 好視多眼用懸浮液1公絲/公撮 FOXONE OPHTHALMIC SUSPENSION 1MG/ML "WINSTON" (衛署藥製字第044167號)」(批號 FX-17019)藥品含有未核准添加之Tropicamide散瞳劑成分藥品,食藥署已於9月13日要求業者啟動回收作業,通知醫療機構及藥局立即下架停止供應,並於1個月內(107年10月13日前)完成回收,請衛生局督導下架回收事宜。請民眾立即停用案內藥品,並立即回診。
我國核准「"溫士頓" 好視多眼用懸浮液1公絲/公撮FOXONE OPHTHALMIC SUSPENSION 1MG/ML "WINSTON" (衛署藥製字第044167號)」藥品,許可證持有廠商及製造廠為溫士頓醫藥股份有限公司,適應症為眼瞼炎、結膜炎、角膜炎、強膜炎、上強膜炎、虹彩炎、虹彩毛樣體炎。此次係檢出Tropicamide成分,該成分屬於散瞳劑,一般使用於眼科檢查及假性近視,可能短暫發生畏光、視力模糊等情形。 為確保藥物安全與醫療效能,食藥署已建置藥物安全監測機制,即時監視國內、外藥物安全訊息,除設有藥物不良反應通報系統及藥物不良品通報中心之外,並對於藥物之安全性與療效亦隨時進行再評估,如醫療人員或病患疑似因使用(服用)藥品導致不良反應之發生,請立即通報衛生福利部所建置之全國藥物不良反應通報中心,藥物不良反應通報專線02-2396-0100,網站:https://adr.fda.gov.tw。如發現藥物不良品時,請立即通報衛生福利部所建置之全國藥物不良品通報中心,藥物不良品通報專線02-6625-1166分機6401,網站: https://qms.fda.gov.tw。  首先,要了解自己一天有本錢吃多少熱量(就是俗稱的每日新陳代謝)。
在減重第一步中,教大家基礎代謝的計算方式,因為基礎代謝約佔一天所消耗熱量的七成,所以只要將基礎代謝除以0.7就可以估算出一天的新陳代謝有多少。 #減重第一步 那有沒有什麼方法可以增加自己的新陳代謝呢? 在臨床上,這是最多減重者問的問題。答案是當然有。下面我將就新陳代謝的角度來分析一些可增加新陳代謝的方法。 新陳代謝主要由三個方面決定,分別是: 一、 基礎代謝(佔約70%) 二、生理活動量(佔約20%) 三、攝食產熱效應(佔約10%) 因此,可從在這三個方面努力來增加整體的新陳代謝。 【一、基礎代謝方面】 所謂的基礎代謝就是維持生理機本活動所需的熱量,例如呼吸、心跳、血液循環、體溫維持等,這是維持生命所需的最基本熱量。在基礎代謝中,主要是由肌肉組織所負責,其次是肝臟、腸胃、腎臟、脾臟、心臟及腦等其他代謝性的器官,如果能夠維持這些器官組織的機能在最旺盛的狀態下,就能讓身體消耗最多的熱量。 而提供這些活性代謝組織所需的營養與能源就是維持這些組織機能的最好方法。 簡單地說,就是多吃營養的食物。 要維持良好的新陳代謝,你必須提供身體營養的食物,而不是只注重在卡路里上(此即營養減肥的原理)。這就好比要讓一台車子效能發揮到最好,除了汽油(熱量)外,潤滑油或機油(維生素與礦物質等營養素)也是不可或缺的,短時間也許看不出來,長時間絕對會有差異。臨床上,常看到很多人想減肥的人只專注在卡路里上,為了減肥常常吃固定缺乏營養與變化的食物,例如每天只以吐司與牛奶為當一餐,或吃蘋果餐,或只吃某些特定的東西,這種只重熱量不管營養的減肥方式,一開始體重或許會瘦,但最後常影響身體整體機能,使新陳代謝降低,導致最後只能越吃越少,且一但停止少吃減肥,體重很快就復胖回去。 提升基礎代謝的方法 簡單地說,就是吃營養價值高的食物。一樣300大卡,三明治等有肉有菜的食物優於蛋糕或奶茶等營養價值低的食物。 1、用胚芽米、五穀飯或糙米飯來取代白米飯。 2、用全麥、黑麥或五穀麵包(吐司)取代白麵包或白吐司。 3、以陽春麵搭配一顆蛋或一盤豆乾來取代麻醬麵、涼麵或乾麵。 4、以飯+烤或滷或蒸肉類+菜的均衡組合來取代炒飯、炒麵、義大利奶油麵等單一組合。 5、不要用單一食物減肥法減肥(如只吃蘋果,只喝蔬菜湯,只吃肉類或其他缺乏變化的減肥食物)。 6、每餐有飯有肉有菜,不要以吐司,蘇打餅乾、水果或代餐來取代正餐。 (註:減重代餐一天只建議吃一次) 【二、生理活動方面】 所謂的生理活動包括一般活動(如走路,爬樓梯,做家事),以及我們俗稱的跑步,游泳與運動。雖然一般生理活動每小時所消耗的熱量較少,但因能持續較久的時間,所以累績下來所消耗的熱量有時反而會比從事運動高。舉例來說,慢跑所消耗的熱量雖然比快走多,但慢跑無法持續太久。 但快走卻很容易持續數十分到數小時的時間(相信很多女性同胞都有以”時”計的壓馬路習慣)。 這裡並非反對運動,或是說運動沒有效,而是希望大家把觀念著重在過"好動"的生活,也就是增加一般的生理活動量,而非過度執著於找時間去做運動,結果流於沒有時間,僅止於”想”的程度。 提升生理活動的方法 如果真的不容易養成運動的習慣(可能是沒時間,缺乏人陪無法持續或其他),你可以選擇養成好動的習慣,例如: 1、以騎單車來取代騎機車或開車。 2、用走路去買三餐或買東西。 3、 養成固定的打掃習慣。 4、用爬樓梯來取代電梯。 5、 提早一至兩站下車或將車停遠一點,增加走路活動的機會。 6、多幫忙做家事或幫忙蹓狗等。 7、 飯後到學校操場,公園綠地或堤防等地方散散步。 8、 假日多從事好動的活動,如登山露營,踏青郊遊,逛家壓馬路。 9、找運動夥伴,固定從事運動(如打球,游泳等)。 記得,勿以”動少”而不為,積少成多這是提升生理活動的座右銘。 【三、食物攝食產熱效應】 所謂的食物攝食產熱效應是指食物攝食過程中消化吸收等過程所消耗的能量,基本上,佔新陳代謝的10%左右。吃越精緻的食物所需要用來消化的熱量越少,吃越粗糙的食物,用來消化吸收所需的熱量越多。 提升食物攝食產熱效應的方法 1、減少油脂的攝取(少吃油炸或油膩的食物)。每吃100大卡的油脂有97大卡會轉變為脂肪儲存,所消耗的熱量最少。 2、以胚芽米、五穀飯或糙米飯來取代白米飯。 3、以瘦肉來取代絞肉。 4、多吃蔬菜水果,少吃餅乾等精緻加工的食物。 5、以新鮮水果來取代果汁。 6、不要喝含糖飲料或濃湯等較不需消化的食物。  正常落髮:平均每日掉髮約100-150根,落髮量與年紀有關。 (不用過度擔心) 1、家族史:是否有掉髮的家族遺傳史 2、抓髮測試:以手指抓取一小掫約25到30根,稍施力拉超過6根脫落為異常 3、圈髮測試:用拇指與食指將所有的頭髮往後圈成馬尾,直徑小於10元銅板 4、枕頭落髮量:平均每天落髮在枕頭上超過35根為異常 5、觀察髮根:髮根無透明毛囊內鞘,為異常角化現象 6、髮際線:前額左右兩側頭髮掉落,髮際線往後退 雄性禿可說是最悲慘的掉髮族群,因為命運的枷鎖讓自己逃都逃不掉。
有雄性禿基因者有高達1/3的機會會禿髮,原因在於雄性荷爾蒙如果代謝成二氫睪固酮,會讓毛囊萎縮,通常在 30多歲至40歲間濃度會很高,若壓力大或熬夜可能濃度會更高,造成落髮的情形就會更嚴重。 至於有家族史者會不會提早發生難定論,平時可以請自己的髮型師幫忙注意,尤其男生很少換髮型師,因此當髮型師覺得你的頭髮變少時就要去看診,另外,髮線愈來愈高,從眉毛往上8、9公分以上就得注意了。 有禿髮基因的人無論男女,總會在某個點,例如壓力大、睡眠不足、飲食不正常後,突然開始大量掉髮,就像掀開了潘朵拉的盒子一發不可收拾。 簡銘成醫師提醒民眾有三大徵兆要注意。 第一型:區塊(島嶼狀分佈)掉髮: 有些區塊(島嶼狀分佈)沒有頭髮,無論是圓型禿、黴菌感染或瘢痕性掉髮,這些問題都是頭皮頭髮生病了得趕快就醫,找到原因後,只要毛囊沒有完全破壞,是有可能恢復的。 第二型:短期掉髮數量明顯增加: 是掉髮數量明顯增加,平常可能只有掉十幾根髮,突然一次掉2、30根,主要是頭髮大量進入休止期。簡銘成醫師說,這個徵兆頭皮可能沒事,但要找出原因得回顧病人的病史,例如生產後、開完刀或經歷重大事件後發生。時間是最好的解決方式,塗養髮液可以加速復原。 第三型:型態性掉髮,M型或是地中海型: 這是最常見的雄性禿或女性掉髮。這類患者掉髮是在「無形」中增加,簡銘成形容,就像溫水煮青蛙,一次增加十根掉髮,根本不會在意,等發現時恐怕已進入雄性禿第三期了。 最後提醒雄性禿的朋友,確診有雄性禿的情況,請勿自行斷藥,該口服藥或外用藥治療還是要遵照醫師藥師指示,正確使用藥品。 權威醫學雜誌-新英格蘭醫學雜誌 (NEJM),在2018年8月26日,發表了 Lorcaserin (沛麗婷 Belviq® ) 的心血管風險研究結果。 直接先說重點 (研究結果) 1、服用 Lorcaserin 能明顯減重。 2、Lorcaserin 並不會顯著增加主要心血管事件 (如:心因性死亡、心肌梗塞、中風等) 的發生率。 3、有肥胖合併糖尿病者,同時使用 Lorcaserin 及降血糖藥物 (如:胰島素、sulfonylurea 類藥物),需特別小心發生低血糖。 參考資料 Cardiovascular Safety of Lorcaserin in Overweight or Obese Patients. E.A. Bohula, S.D. Wiviott, D.K. McGuire, S.E. Inzucchi, J. Kuder, K.A. Im,C.L. Fanola, A. Qamar, C. Brown, A. Budaj, A. Garcia‐Castillo, M. Gupta, L.A. Leiter, N.J. Weissman, H.D. White, T. Patel, B. Francis, W. Miao, C. Perdomo, S. Dhadda, M.P. Bonaca, C.T. Ruff, A.C. Keech, S.R. Smith, M.S. Sabatine, and B.M. Scirica, for the CAMELLIA–TIMI 61 Steering Committee and Investigators. August 26, 2018, at NEJM.org.   減重第二迷思:減重就都不要吃澱粉?
講到減重或減肥,很多人的第一印象就是不能吃澱粉,事實上,這是絕對錯誤的觀念。澱粉(或稱主食類食物或醣類),我們全身有超過60兆細胞都需要澱粉類來供給能量。我們吃的澱粉進到體內會被消化酵素分解,最後以葡萄糖的形式存在血液中[也就是血糖],這些糖分會隨著血液運送到全身,提供全身細胞能量使用。 故若你不吃澱粉,會使血糖太低,此時你將會發現全身無力,大腦混沌無法思考,情緒暴躁等各式低血糖現象….這都是身體在告訴你(細胞在呼喚)它需要糖,故即使是減肥,也該吃澱粉,不吃澱粉是錯誤的觀念。 關鍵不在澱粉,而是吃了過量或過度加工的食物! 為什麼有很多人說不可以吃澱粉呢?主要是因為現代人吃了太多糖類食物,如吃澱粉時額外加了很多其他的料,或吃了很多含精緻糖的加料食物: 吃炒飯、炒麵等加了很多油烹調的澱粉類食物。一湯匙油(約135大卡)就有半碗飯的熱量,如果你曾經觀察過炒飯炒麵等所放的油,會發現一大湯匙的油加進去,為炒飯炒麵多加了數百大卡的熱量。 吃滷肉飯、雞肉飯、乾麵、叉燒飯等,額外加了很多油的主食類食物。一樣等於在這些食物額外加了上百卡的熱量。 餅乾糕點等額外加油加糖的食物吃太多。不管是中式糕點或西式甜點,多半額外加了很多糖,或是油脂類的成分。只要翻翻糕點類的食譜,很容易就可發現其中加料還真不少,難怪常常一小塊熱量就逼近或是超過一碗飯的熱量。 吐司、法國麵包、饅頭吃太多。很多人會為了減肥而特別挑選吐司饅頭等感覺較不油與不甜的東西,殊不知這類食物相當扎實,往往一小點熱量就可媲美白飯,而又不向白飯般會搭配肉類與蔬菜等食物吃,故往往吃不飽,因此若吃太多很容易變胖。[註:一般便利商店的吐司一片約1.5~2份主食,約100~140大卡;法國麵包兩指寬約一份主食,70大卡;饅頭一個拳頭大就有約四份主食,280大卡熱量] 含糖飲料喝太多。很多人不喜歡喝白開水,而喜歡喝有味道的飲料,從便利商店的各式鋁箔包與罐裝飲料,到現打的果汁、現搖的泡沫紅茶或奶茶,或標榜健康訴求的優酪乳、多多。這類食物多半添加了很多額外的糖與加料成份,故喝多了很容易胖起來。[註:一般飲料要讓人感到甜,約有10%左右的糖,故500cc的飲料約含50公克糖,也就是就有200大卡的熱量] 生酮飲食讓澱粉類食物被污名化! 有人主張減肥時不吃澱粉(這種方法又稱為生酮飲食),故很多人講到減肥就會想到不能吃澱粉,事實上這也是誤會了澱粉,將澱粉污名化。 事實上,不吃澱粉減肥(吃肉減肥)所利用得原理就是澱粉所提供的糖類是細胞主要能量來源,故透過強制不提供澱粉給身體,讓身體為了維持血糖、提供細胞能量,轉而將蛋白質和脂肪兩類營養素轉化為醣類,提供給身體使用(在營養學上這個機轉叫做"醣質新生作用")。這個方法之可以瘦就出現在這個強制過程中的代謝反應:蛋白質轉化過程會產生含氮廢物,脂肪在缺乏醣類時會因燃燒不完全而產生大量酮酸,身體為了排除這些有毒廢物,會使用大量的水分,將它們從尿中排除出去,因此會有所謂的脫水利尿作用,正因為水份排除,讓人感覺重量降得很快。 這種方法實際減的脂肪相當有限,體重減得快主要是因為水分流失所致,故即使輕了很多,尺寸不見得變化很大。另外有用過的人都會有經驗,當停止使用吃肉減肥時,或在吃肉減肥過程中不小心多吃了澱粉,都會讓體重很快又回復,這也是因為攝取到澱粉後,身體代謝恢復正常,不會有過多有毒廢物產生,不會發生利尿作用,之前的水分又回到身體來,故體重恢復回來所致。澱粉在其中並非導致發胖或讓你無法減肥的緣故,它只是不小心被誤解,污名化而已。 @正確選用,吃澱粉不怕胖! 一.適「質」,選對澱粉吃不胖! * 飯類:糙米飯、胚芽米飯、雜糧飯等最好,白米飯和糯米其次。將飯煮成稀飯後,因為米粒吸水膨脹,所以容易飽但熱量低,一般而言,吃兩碗稀飯才只有一碗乾飯的熱量而已。飯本身沒問題,只要不要額外加油汁、肉汁、醬汁或用油去炒即可。 * 麵食類:如簥麥麵,麵條,麵線,米粉,冬粉等。麵食類因為吸水膨脹,所以在同體積下熱量較飯類低。因此,如果比較餓的話,可以盡量挑這類食物,吃起來容易飽,熱量又不高。其中冬粉、米粉的熱量又略低於麵線與麵。同樣,本身不是問題,烹調過程不要有額外的油或吃時額外加油脂(香油、辣油、麻油、麻醬等)就沒問題。 * 五穀雜糧類:如紅豆、綠豆、大麥等五穀雜糧,此類食物具較高的營養價值,且含較多的纖維,吃了容易飽,可以說是非常適合想減肥的人。但是因為大多以甜食的方式供應,所以反而因為糖的問題,使它的好打了折扣,建議若想吃甜的時,可以用代糖取代砂糖。 * 根莖類:如地瓜,馬鈴薯,南瓜,山藥,玉米等食物。此類食物含豐富的維生素及纖維,也是很適合想減肥者的健康食物,但因為可能有烹調的油或糖的問題,所以吃的時候要注意。此外,這類食物體積小,熱量不低,幾乎等同飯類,故吃了後就不宜再吃飯或應該減少原本飯麵的食用量,不然容易過食。 二.適「量」,吃進來用得掉不會胖! 葡萄糖(澱粉類食物吃到體內後所分解而成的最小單位)是我們大腦與神經唯一的能量來源,所以澱粉類食物吃進來是先被身體以能量的形式拿來用,多餘的才會轉變成脂肪儲存起來,因此只要吃的量剛好在身體所能用掉的範圍內,是吃不胖的。 另外值得一提的是,最近有一篇文章 不吃澱粉恐早死! 可以點閱參考一下。 |
依主管機關相關規定,專業醫藥資訊僅提供醫藥專業人員參考(請申請核可通過後,即可閱讀專業人員區)。
恕不對外開放非專業人士使用。 每月文章
一月 2023
類別 |










 RSS 訂閱
RSS 訂閱
營業時間:週一至週日(全年無休) 早上九點至晚上十一點四十分 (09:00~23:40)
|
地址:台北市松山區饒河街204號
|
聯絡我們
|